Department of Medical, Surgical, Neurological, Metabolic and Aging Sciences, University of Campania "Luigi Vanvitelli", Piazza Miraglia, 2, 80138, Naples, Italy.
Cardiovascular and Arrhythmias Department, John Paul II Research and Care Foundation, Campobasso, Italy.
Cardiovasc Diabetol. 2018 Oct 22;17(1):137. doi: 10.1186/s12933-018-0778-9.
To evaluate clinical outcomes in patients with diabetes, treated by cardiac resynchronization therapy with a defibrillator (CRT-d), and glucagon-like peptide 1 receptor agonists (GLP-1 RA) in addition to conventional hypoglycemic therapy vs. CRTd patients under conventional hypoglycemic drugs.
Patients with diabetes treated by CRTd experienced an amelioration of functional New York Association Heart class, reduction of hospital admissions, and mortality, in a percentage about 60%. However, about 40% of CRTd patients with diabetes experience a worse prognosis.
We investigated the 12-months prognosis of CRTd patients with diabetes, previously treated with hypoglycemic drugs therapy (n 271) vs. a matched cohort of CRTd patients with diabetes treated with GLP-1 RA in addition to conventional hypoglycemic therapy (n 288).
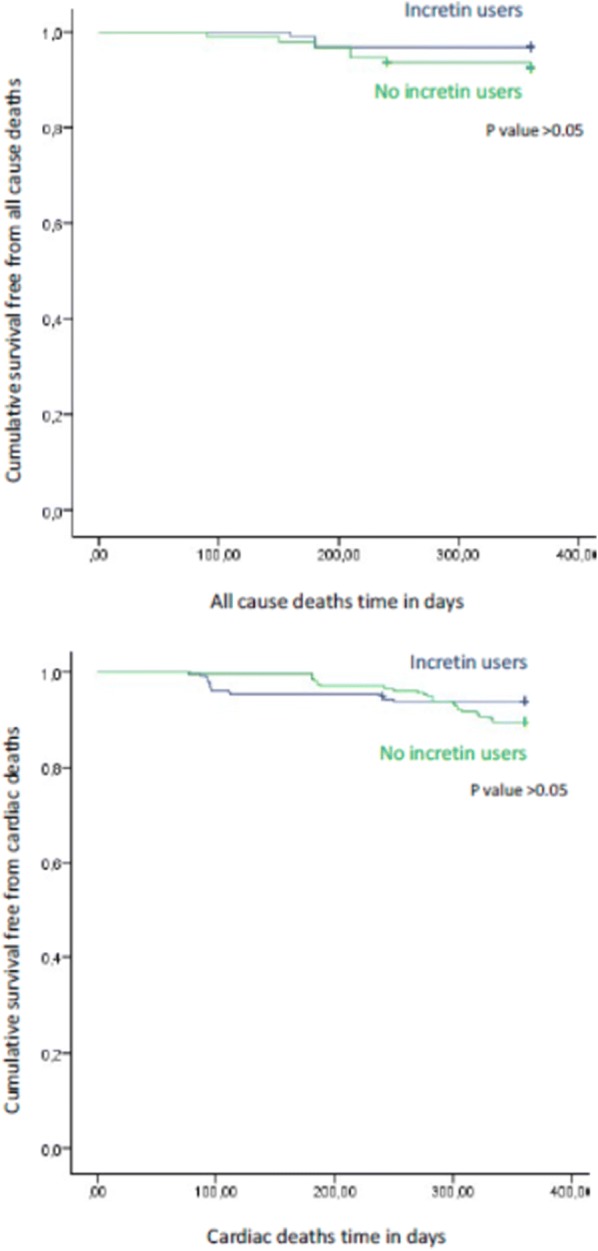
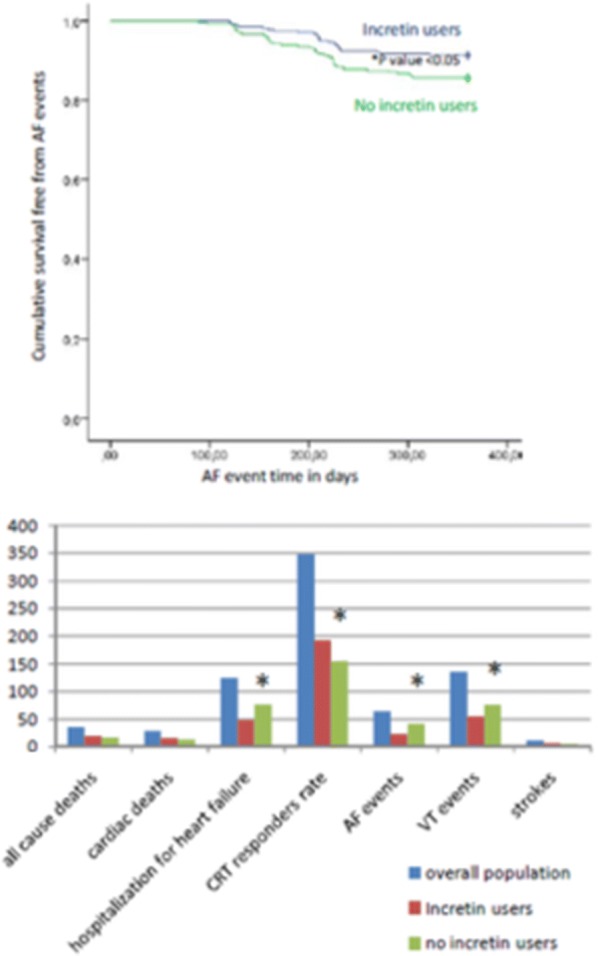
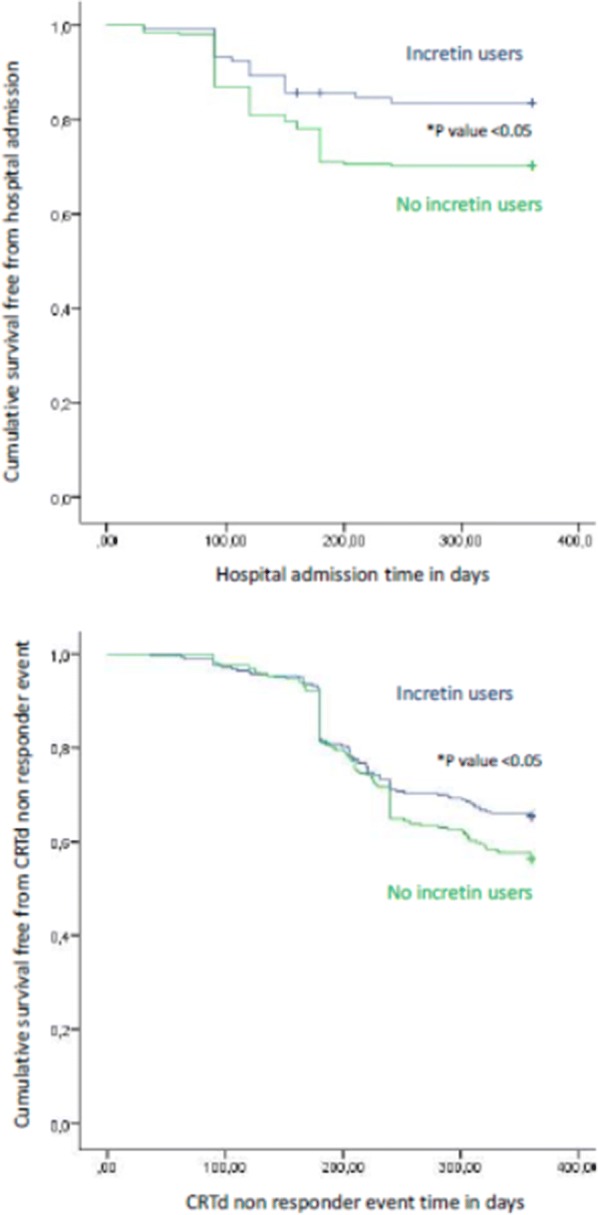
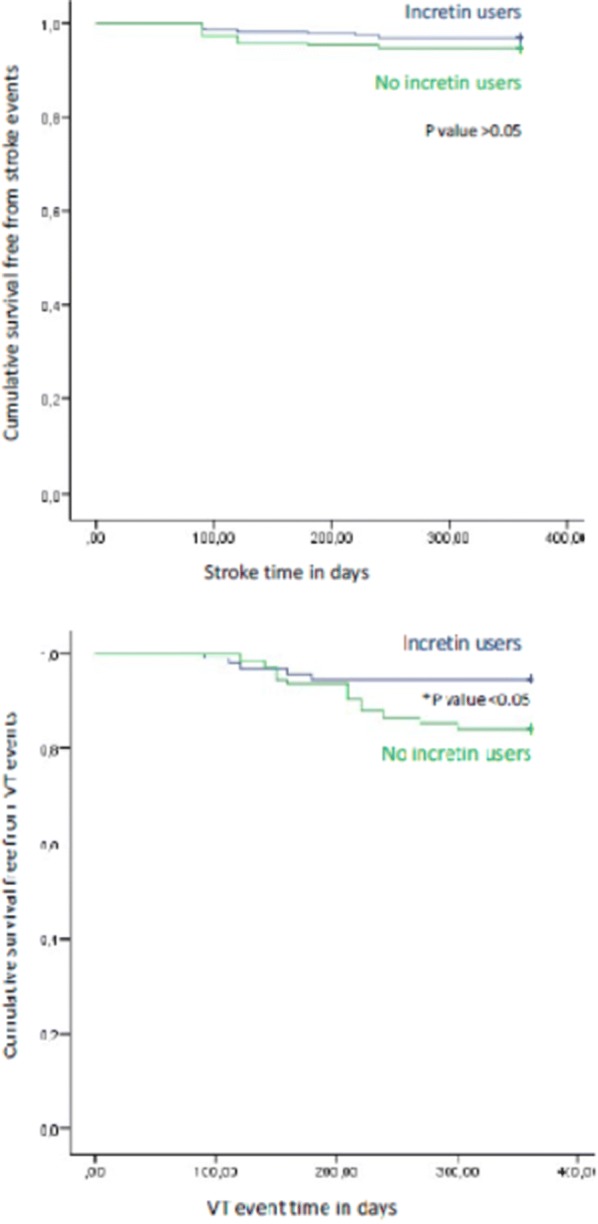
At follow up CRTd patients with diabetes treated by GLP-1 RA therapy vs. CRTd patients with diabetes that did not receive GLP-1 RA therapy, experienced a significant reduction of NYHA class (p value < 0.05), associated to higher values of 6 min walking test (p value < 0.05), and higher rate of CRTd responders (p value < 0.05). GLP-1 RA patients vs. controls at follow up end experienced lower AF events (p value < 0.05), lower VT events (p value < 0.05), lower rate of hospitalization for heart failure worsening (p value < 0.05), and higher rate of CRTd responders (p value < 0.05). To date, GLP-1 RA therapy may predict a reduction of AF events (HR 0.603, CI [0.411-0.884]), VT events (HR 0.964, CI [0.963-0.992]), and hospitalization for heart failure worsening (HR 0.119, CI [0.028-0.508]), and a higher CRT responders rate (HR 3.707, CI [1.226-14.570]).
GLP-1 RA drugs in addition to conventional hypoglycemic therapy may significantly reduce systemic inflammation and circulating BNP levels in CRTd patients with diabetes, leading to a significant improvement of LVEF and of the 6 min walking test, and to a reduction of the arrhythmic burden. Consequently, GLP-1 RA drugs in addition to conventional hypoglycemic therapy may reduce hospital admissions for heart failure worsening, by increasing CRTd responders rate. Trial registration NCT03282136. Registered 9 December 2017 "retrospectively registered".
评估患有糖尿病的患者在接受心脏再同步治疗除颤器(CRT-d)和胰高血糖素样肽 1 受体激动剂(GLP-1RA)治疗的临床结果,以及接受传统降糖药物治疗的患者与接受传统降糖药物治疗的 CRT-d 患者相比。
接受 CRT-d 治疗的糖尿病患者的纽约心脏协会功能分级改善,住院和死亡率降低,比例约为 60%。然而,约 40%的糖尿病 CRT-d 患者预后较差。
我们研究了先前接受降糖药物治疗(n=271)的 CRT-d 糖尿病患者与接受 GLP-1RA 联合常规降糖治疗的 CRT-d 糖尿病患者(n=288)的 12 个月预后。
在随访中,接受 GLP-1RA 治疗的 CRT-d 糖尿病患者与未接受 GLP-1RA 治疗的 CRT-d 糖尿病患者相比,NYHA 分级显著降低(p 值<0.05),6 分钟步行试验的结果更高(p 值<0.05),并且 CRT-d 反应者的比例更高(p 值<0.05)。随访结束时,GLP-1RA 患者与对照组相比,心房颤动(AF)事件(p 值<0.05)、室性心动过速(VT)事件(p 值<0.05)、心力衰竭恶化住院率(p 值<0.05)较低,且 CRT-d 反应者比例较高(p 值<0.05)。到目前为止,GLP-1RA 治疗可能降低 AF 事件(HR 0.603,CI [0.411-0.884])、VT 事件(HR 0.964,CI [0.963-0.992])和心力衰竭恶化住院率(HR 0.119,CI [0.028-0.508]),并提高 CRT-d 反应者的比例(HR 3.707,CI [1.226-14.570])。
GLP-1RA 药物联合常规降糖治疗可显著降低糖尿病 CRT-d 患者的全身炎症和循环 BNP 水平,显著改善 LVEF 和 6 分钟步行试验,并降低心律失常负担。因此,GLP-1RA 药物联合常规降糖治疗可能通过提高 CRT-d 反应者的比例来降低心力衰竭恶化的住院率。试验注册 NCT03282136。于 2017 年 12 月 9 日“回顾性注册”。