Sardu Celestino, Barbieri Michelangela, Santamaria Matteo, Giordano Valerio, Sacra Cosimo, Paolisso Pasquale, Spirito Alessandro, Marfella Raffaele, Paolisso Giuseppe, Rizzo Maria Rosaria
Department of Medical, Surgical, Neurological, Metabolic and Aging Sciences, University of Campania "Luigi Vanvitelli", Piazza Miraglia, 2, 80138, Naples, Italy.
Cardiovascular and Arrhythmias Department, John Paul II Research and Care Foundation, Campobasso, Italy.
Cardiovasc Diabetol. 2017 Jun 9;16(1):75. doi: 10.1186/s12933-017-0554-2.
Type 2 diabetes mellitus (T2DM) is a multi factorial disease, affecting clinical outcomes in failing heart patients treated by cardiac resynchronization therapy with a defibrillator (CRT-d).
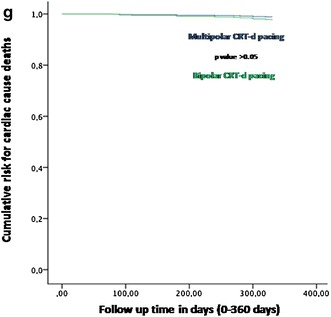
One hundred and ninety-five T2DM patients received a CRT-d treatment. Randomly the study population received a CRT-d via multipolar left ventricle (LV) lead pacing (n 99, multipolar group), vs a CRT-d via bipolar LV pacing (n 96, bipolar group). These patients were followed by clinical, and instrumental assessment, and telemetric device control at follow up. In this study we evaluated, in a population of failing heart T2DM patients, cardiac deaths, all cause deaths, arrhythmic events, CRT-d responders rate, hospitalizations for HF worsening, phrenic nerve stimulation (PNS), and LV catheter dislodgment events (and re-intervention for LV catheter re-positioning), comparing multipolar CRT-d vs bipolar CRT-d group of patients at follow up.
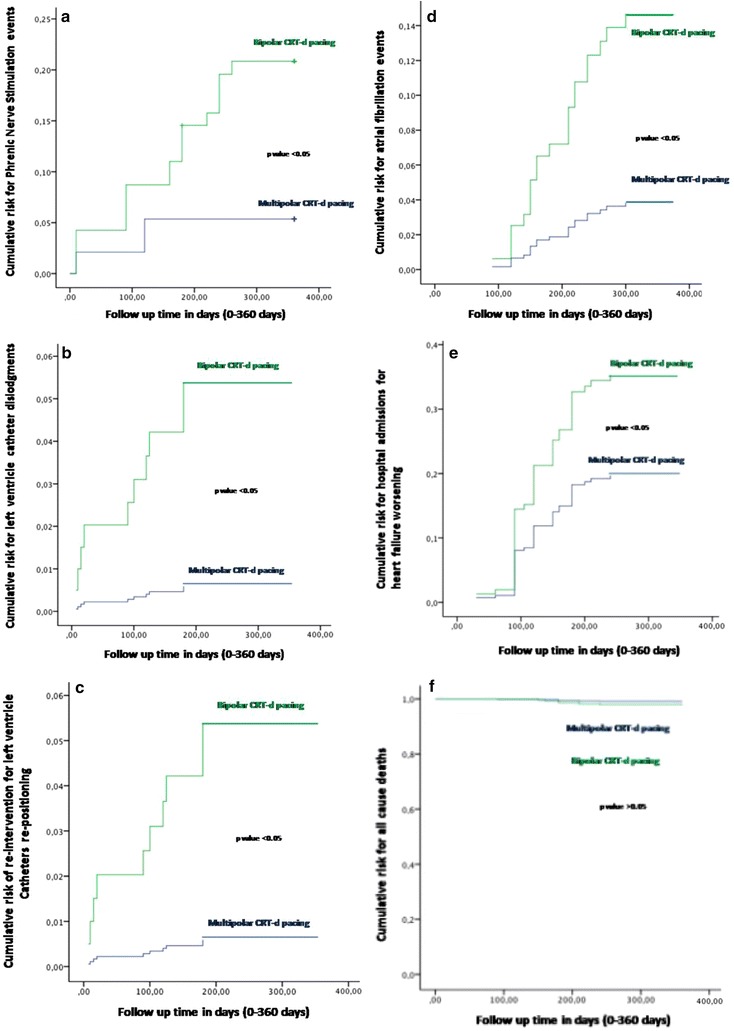
At follow up there was a statistical significant difference about atrial arrhythmic events [7 (7%) vs 16 (16.7%), p value 0.019], hospitalizations for HF worsening [15 (15.2% vs 24 (25%), p value 0.046], LV catheter dislodgments [1 (1%) vs 9 (9.4%), p value 0018], PNS [5 (5%) vs 18 (18.7%), p value 0.007], and LV re-positioning [1 (1%) vs 9 (9.4%), p value 0.018], comparing multipolar CRT-d vs bipolar CRT-d group of patients. Multipolar pacing was an independent predictor of all these events.
CRT-d pacing via multipolar LV lead vs bipolar LV lead may reduce arrhythmic burden, hospitalization rate, PNS, LV catheters dislodgments, and re-interventions in T2DM failing heart patients. Clinical trial number NCT03095196.
2型糖尿病(T2DM)是一种多因素疾病,会影响接受心脏再同步化治疗除颤器(CRT-d)治疗的心力衰竭患者的临床结局。
195例T2DM患者接受了CRT-d治疗。研究人群随机分为通过多极左心室(LV)导线起搏接受CRT-d治疗的患者(n = 99,多极组)和通过双极LV起搏接受CRT-d治疗的患者(n = 96,双极组)。对这些患者进行临床和器械评估,并在随访时进行遥测设备控制。在本研究中,我们评估了心力衰竭T2DM患者群体中的心脏死亡、全因死亡、心律失常事件、CRT-d反应者率、因心力衰竭恶化住院、膈神经刺激(PNS)和LV导管移位事件(以及LV导管重新定位的再次干预),比较了随访时多极CRT-d组与双极CRT-d组患者。
随访时,多极CRT-d组与双极CRT-d组患者在房性心律失常事件[7例(7%)对16例(16.7%),p值0.019]、因心力衰竭恶化住院[15例(15.2%)对24例(25%),p值0.046]、LV导管移位[1例(1%)对9例(9.4%),p值0.018]、PNS[5例(5%)对18例(18.7%),p值0.007]和LV重新定位[1例(1%)对9例(9.4%),p值0.018]方面存在统计学显著差异。多极起搏是所有这些事件的独立预测因素。
与双极LV导线相比,通过多极LV导线进行CRT-d起搏可能会降低T2DM心力衰竭患者的心律失常负担、住院率、PNS、LV导管移位和再次干预。临床试验编号NCT03095196。