Department of Surgery, University of California Los Angeles, Los Angeles, CA, 90095, USA.
Department of Surgery, VA Greater Los Angeles Healthcare System, Los Angeles, CA, 90073, USA.
J Gastrointest Surg. 2019 Jul;23(7):1392-1400. doi: 10.1007/s11605-018-4011-7. Epub 2018 Oct 23.
Patients with early-stage pancreatic neuroendocrine tumors (PNETs) may develop metastatic recurrences despite undergoing potentially curative pancreas resections. We sought to identify factors predictive of metastatic recurrences and develop a prognostication strategy to predict recurrence-free survival (RFS) in resected PNETs.
Patients with localized PNETs undergoing surgical resection between 1989 and 2015 were identified. Univariate and multivariate analysis were used to identify potential predictors of post-resection metastasis. A score-based prognostication system was devised using the identified factors. The bootstrap model validation methodology was utilized to estimate the external validity of the proposed prognostication strategy.
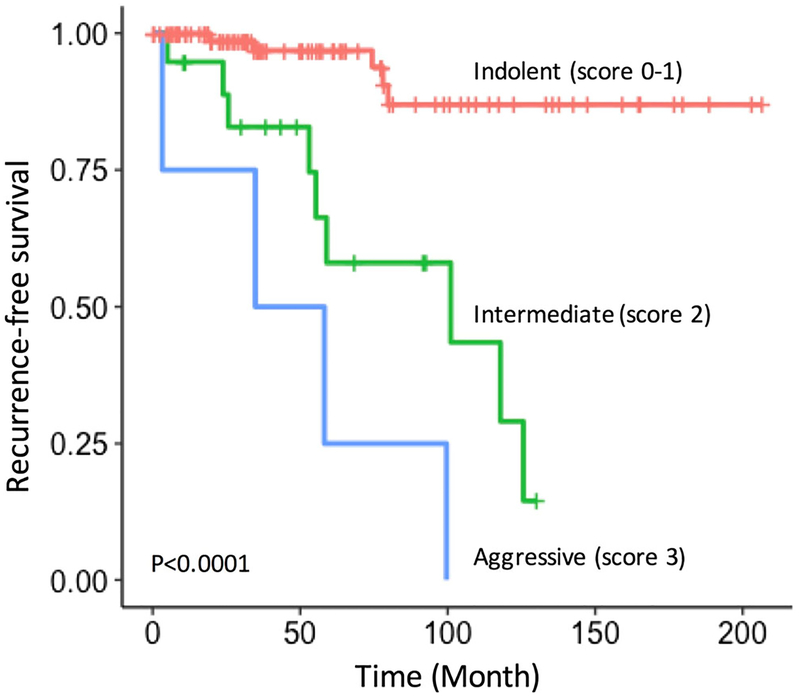
Of the 140 patients with completely resected early-stage PNETs, overall 5- and 10-year RFS were 84.6% and 67.1%, respectively. The median follow-up was 56 months. Multivariate analysis identified tumor size > 5 cm, Ki-67 index 8-20%, lymph node involvement, and high histologic grade (G3, or Ki-67 > 20%) as independent predictors of post-resection metastatic recurrence. A scoring system based on these factors stratified patients into three prognostic categories with distinct 5-year RFS: 96.9%, 54.8%, and 33.3% (P < 0.0001). The bootstrap model validation methodology projected our proposed prognostication strategy to retain a high predictive accuracy even when applied in an external dataset (validated c-index of 0.81).
The combination of tumor size, LN status, grade, and Ki-67 was identified as the most highly predictive indicators of metastatic recurrences in resected PNETs. The proposed prognostication strategy may help stratify patients for adjuvant therapies, enhanced surveillance protocols and future clinical trials.
尽管接受了可能治愈的胰腺切除术,早期胰腺神经内分泌肿瘤(PNETs)患者仍可能发生转移性复发。我们试图确定预测转移性复发的因素,并制定预测胰腺神经内分泌肿瘤切除后无复发生存率(RFS)的预后策略。
确定了 1989 年至 2015 年间接受手术切除的局限性 PNET 患者。使用单因素和多因素分析来确定术后转移的潜在预测因素。使用确定的因素设计基于评分的预后系统。使用引导模型验证方法来估计所提出的预后策略的外部有效性。
在 140 例完全切除的早期 PNET 患者中,总 5 年和 10 年 RFS 分别为 84.6%和 67.1%。中位随访时间为 56 个月。多因素分析确定肿瘤大小>5cm、Ki-67 指数 8-20%、淋巴结受累和高组织学分级(G3,或 Ki-67>20%)是术后转移复发的独立预测因素。基于这些因素的评分系统将患者分为三个具有不同 5 年 RFS 的预后类别:96.9%、54.8%和 33.3%(P<0.0001)。引导模型验证方法预测,即使在外部数据集(验证的 c 指数为 0.81)中应用,我们提出的预后策略仍保留较高的预测准确性。
肿瘤大小、LN 状态、分级和 Ki-67 的组合被确定为预测胰腺神经内分泌肿瘤切除后转移复发的最具预测性指标。所提出的预后策略可能有助于分层患者进行辅助治疗、增强监测方案和未来的临床试验。