Lemiengre Marieke B, Verbakel Jan Y, Colman Roos, Van Roy Kaatje, De Burghgraeve Tine, Buntinx Frank, Aertgeerts Bert, De Baets Frans, De Sutter An
a Department of Public Health and Primary Care , Ghent University , Ghent , Belgium.
b Nuffield Department of Primary Care Health Sciences , University of Oxford , Oxford , UK.
Scand J Prim Health Care. 2018 Dec;36(4):423-436. doi: 10.1080/02813432.2018.1529900. Epub 2018 Oct 25.
Antibiotics are prescribed too often in acutely ill children in primary care. We examined whether a Point-of-Care (POC) C-reactive Protein (CRP) test influences the family physicians' (FP) prescribing rate and adherence to the Evidence Based Medicine (EBM) practice guidelines.
Cluster randomized controlled trial.
Primary care, Flanders, Belgium.
Half of the children with non-severe acute infections (random allocation of practices to perform POC CRP or not) and all children at risk for serious infection were tested with POC CRP.
Acutely ill children consulting their FP.
Immediate antibiotic prescribing.
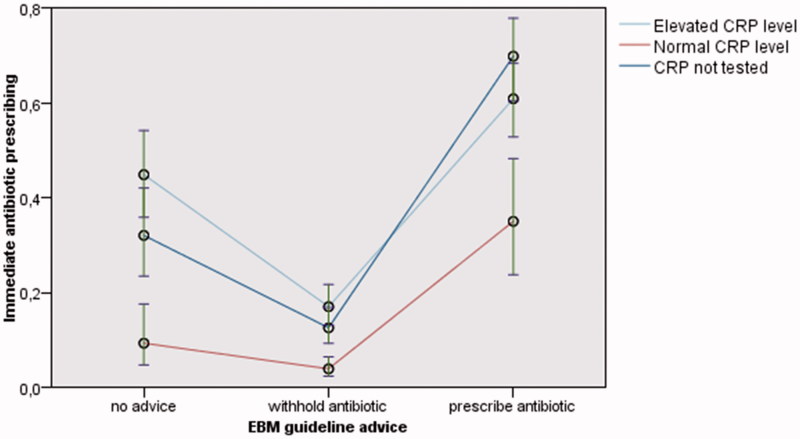
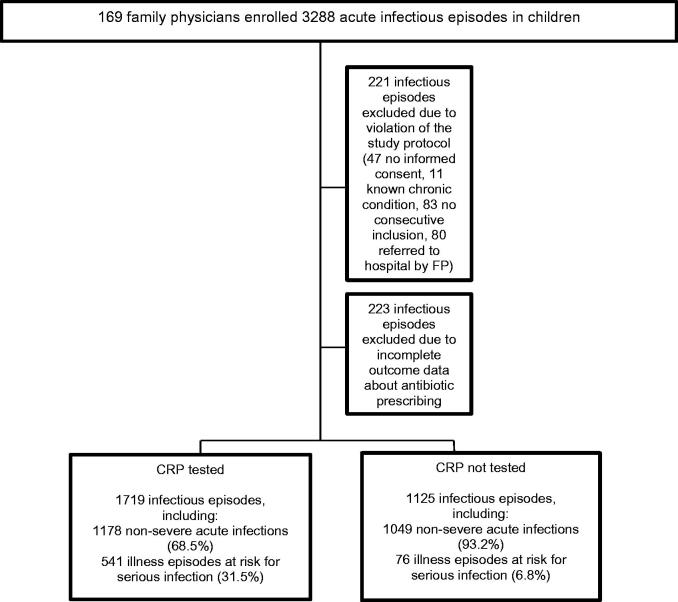
2844 infectious episodes recruited by 133 FPs between 15 February 2013 and 28 February 2014 were analyzed. A mixed logistic regression analysis was performed. Compared to episodes in which CRP was not tested, the mere performing of POC CRP reduced prescribing in case EBM practice guidelines advise to prescribe antibiotics (adjusted odds ratio (aOR) 0.54 (95% Confidence Interval (CI) 0.33-0.90). Normal CRP levels reduced antibiotic prescribing, regardless of whether the advice was to prescribe (aOR 0.24 (95%CI 0.11-0.50) or to withhold (aOR 0.31 (95%CI 0.17-0.57)). Elevated CRP levels did not increase antibiotic prescribing.
Normal CRP levels discourage immediate antibiotic prescribing, even when EBM practice guidelines advise differently. Most likely, a normal CRP convinces FPs to withhold antibiotics when guidelines go against their own gut feeling. Future research should focus on whether POC CRP can effectively identify children that benefit from antibiotics more accurately, without increasing the risks of under-prescribing. Key points What is previously known or believed on this topic •Antibiotics are prescribed too often for non-severe conditions. Point-of-care (POC) C-reactive Protein (CRP) testing without guidance does not reduce immediate antibiotic prescribing in acutely ill children in primary care. What this research adds •FPs clearly consider CRP once available: normal CRP levels discourage immediate antibiotic prescribing, even when EBM practice guidelines advise differently. Most likely, a normal CRP convinces FPs to withhold antibiotics when guidelines go against their own gut feeling. •Future research should focus on whether POC CRP can effectively identify children that benefit from antibiotics more accurately, without increasing the risks of under-prescribing.
在基层医疗中,急性病患儿抗生素使用过于频繁。我们研究了即时检验(POC)C反应蛋白(CRP)检测是否会影响家庭医生(FP)的抗生素处方率以及对循证医学(EBM)实践指南的遵循情况。
整群随机对照试验。
比利时弗拉芒大区的基层医疗。
对一半患有非严重急性感染的儿童(通过随机分配诊所决定是否进行POC CRP检测)以及所有有严重感染风险的儿童进行POC CRP检测。
向家庭医生咨询的急性病患儿。
即时抗生素处方。
分析了2013年2月15日至2014年2月28日期间133名家庭医生招募的2844次感染发作情况。进行了混合逻辑回归分析。与未检测CRP的发作情况相比,仅进行POC CRP检测在EBM实践指南建议使用抗生素的情况下减少了处方(调整优势比(aOR)0.54(95%置信区间(CI)0.33 - 0.90))。正常的CRP水平降低了抗生素处方,无论指南建议是使用(aOR 0.24(95%CI 0.11 - 0.50))还是不使用(aOR 0.31(95%CI 0.17 - 0.57))。CRP水平升高并未增加抗生素处方。
即使EBM实践指南有不同建议,正常的CRP水平也会抑制即时抗生素处方。很可能,当指南与他们自己的直觉相悖时,正常的CRP会使家庭医生不使用抗生素。未来的研究应关注POC CRP是否能在不增加处方不足风险的情况下,更有效地准确识别能从抗生素中获益的儿童。要点关于该主题先前已知或被认为的情况•对于非严重病症,抗生素使用过于频繁。在基层医疗中,无指导的即时检验(POC)C反应蛋白(CRP)检测不会减少急性病患儿的即时抗生素处方。本研究的新增内容•一旦有了CRP结果,家庭医生会明确予以考虑:即使EBM实践指南有不同建议,正常的CRP水平也会抑制即时抗生素处方。很可能,当指南与他们自己的直觉相悖时,正常的CRP会使家庭医生不使用抗生素。•未来的研究应关注POC CRP是否能在不增加处方不足风险的情况下,更有效地准确识别能从抗生素中获益的儿童。