Shanghai Key Laboratory of Diabetes, Department of Endocrinology & Metabolism, Shanghai Jiao-Tong University Affiliated Sixth People's Hospital, Shanghai Clinical Medical Center of Diabetes, Shanghai Key Clinical Center of Metabolic Diseases, Shanghai Institute for Diabetes, 600 Yishan Road, Shanghai, 200233, China.
Department of Obstetrics and Gynecology, Shanghai Clinical Center for Severe Maternal Rescue, Shanghai Jiao-Tong University Affiliated Sixth People's Hospital, Shanghai, China.
J Transl Med. 2018 Oct 24;16(1):289. doi: 10.1186/s12967-018-1666-5.
Insulin resistance and beta cell dysfunction were reported to be responsible for gestational diabetes mellitus (GDM). However, little is known about the heterogeneity of these factors and its influences on perinatal outcomes. We investigated whether subtypes of insulin resistance and beta cell dysfunction in gestational diabetes mellitus have different impacts on perinatal outcomes.
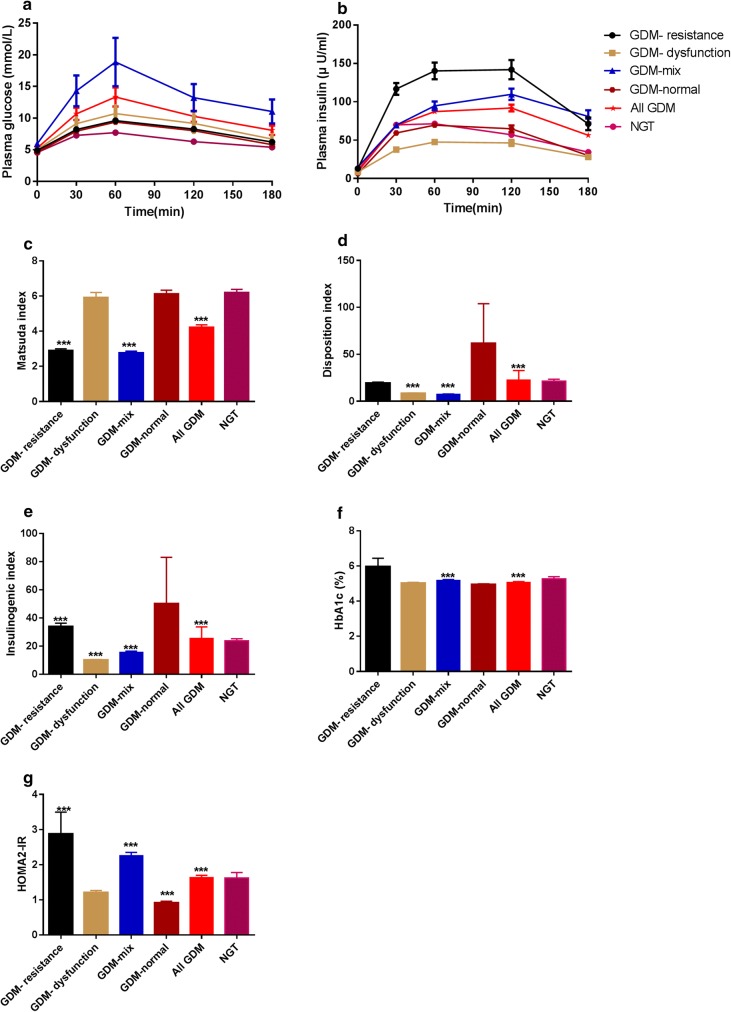
In this prospective cohort study, we followed 554 pregnant women and glucose challenge test was performed at 24-28th weeks of their gestation. Women with plasma glucose ≥ 7.8 mmol/L would be included and advised to undergo the diagnostic 75-g, 3-h oral glucose tolerance test. According to indices of measuring insulin resistance or beta cell function were below the 25th percentile of women with normal glucose tolerance (NGT), women with GDM were defined as three subtypes: GDM with the beta cell dysfunction, GDM with the insulin resistance defect or GDM with both traits mentioned above (GDM-mixed). Perinatal outcomes were documented.
The levels of prepregnancy and maternal BMI in the GDM-mix group were higher compared to women in the NGT group (23.2 ± 4.0 vs 20.8 ± 3.7 kg/m, P < 0.001; 24.5 ± 4.3 vs 21.8 ± 3.4 kg/m, P < 0.001, respectively). Furthermore, women in GDM-mix group more likely to be subjected to LGA (P = 0.008) adverse perinatal outcomes (P = 0.005), although these differences were normalized after adjusting age, prepregnancy and maternal BMI (GDM-mix vs. NGT: P = 0.141 for LGA and P = 0.186 for adverse outcomes). On the other hand, all perinatal outcomes were similar between other two GDM subgroups and NGT group.
Women with GDM display respective characteristics on metabolism disorders and confer discriminating risks of adverse perinatal outcomes because of this heterogeneity.
胰岛素抵抗和β细胞功能障碍被认为是导致妊娠期糖尿病(GDM)的原因。然而,对于这些因素的异质性及其对围产期结局的影响知之甚少。我们研究了妊娠期糖尿病中胰岛素抵抗和β细胞功能障碍的亚组是否对围产期结局有不同的影响。
在这项前瞻性队列研究中,我们随访了 554 名孕妇,在妊娠 24-28 周时进行了葡萄糖挑战试验。血糖≥7.8mmol/L 的妇女将被纳入并建议进行诊断性 75g、3 小时口服葡萄糖耐量试验。根据胰岛素抵抗或β细胞功能的指标低于糖耐量正常(NGT)妇女的第 25 百分位数,将 GDM 妇女定义为三种亚组:β细胞功能障碍型 GDM、胰岛素抵抗缺陷型 GDM 或同时具有上述两种特征的 GDM(GDM-混合型)。记录围产期结局。
与 NGT 组相比,GDM-混合型组的孕前和产妇 BMI 水平更高(23.2±4.0 vs 20.8±3.7kg/m2,P<0.001;24.5±4.3 vs 21.8±3.4kg/m2,P<0.001)。此外,GDM-混合型组的女性更有可能发生巨大儿(P=0.008)和不良围产期结局(P=0.005),尽管这些差异在调整年龄、孕前和产妇 BMI 后趋于正常(GDM-混合型与 NGT:巨大儿为 P=0.141,不良结局为 P=0.186)。另一方面,其他两种 GDM 亚组与 NGT 组的所有围产期结局均相似。
由于这种异质性,GDM 女性在代谢紊乱方面表现出各自的特征,并带来不同的不良围产期结局风险。