Policy Analysis Inc. (PAI), Brookline, Massachusetts, United States.
Bristol-Myers Squibb, Lawrenceville, New Jersey, United States.
Thromb Haemost. 2018 Nov;118(11):1951-1961. doi: 10.1055/s-0038-1673689. Epub 2018 Oct 24.
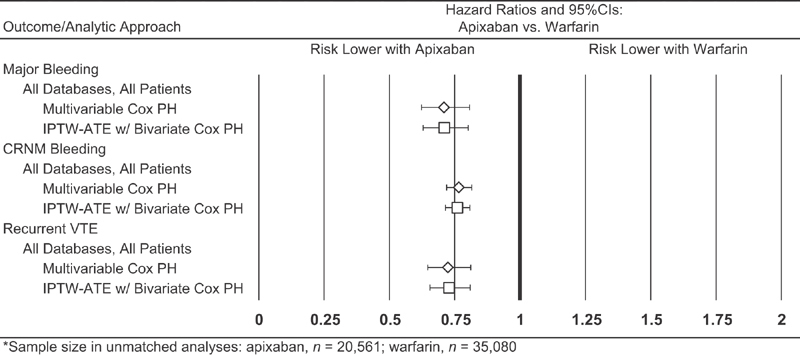
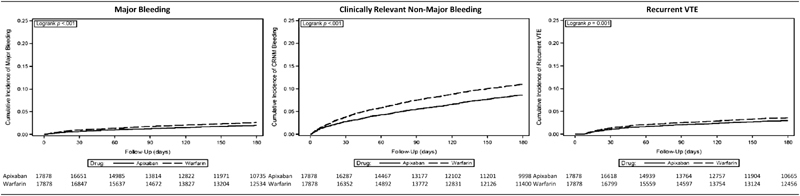
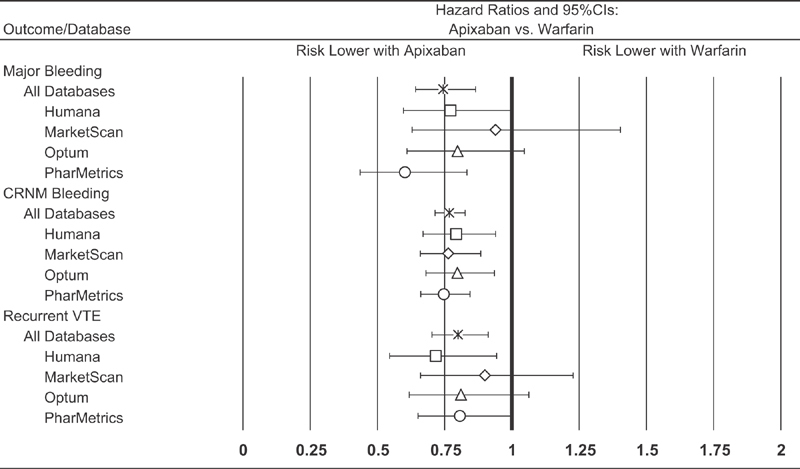
In the AMPLIFY clinical trial, apixaban was non-inferior to warfarin plus subcutaneous enoxaparin bridge therapy in the treatment of acute venous thromboembolism (VTE) and was associated with significantly less bleeding. This study evaluated their comparative effectiveness and safety in routine clinical practice. A matched-cohort design and data from four U.S. private health care claims databases were employed. Study population comprised patients who initiated outpatient treatment with apixaban versus warfarin (plus parenteral anticoagulant bridge therapy) within 30 days of their initial VTE episode; apixaban and warfarin patients were matched on age, characteristics of VTE episode, study database and propensity score. Major bleeding, clinically relevant non-major (CRNM) bleeding and recurrent VTE during the 180-day (maximum) follow-up period were compared using shared frailty models. During mean follow-up of 143 days among apixaban patients ( = 17,878) and 152 days among warfarin patients ( = 17,878), incidence proportions for apixaban versus warfarin, respectively, were 1.7% versus 2.3% for major bleeding, 7.0% versus 9.4% for CRNM bleeding and 2.3% versus 2.9% for recurrent VTE. In shared frailty models, risks of major bleeding (hazard ratio [HR] = 0.75, 95% confidence interval [CI] = 0.64-0.87), CRNM bleeding (HR = 0.77, 95% CI = 0.71-0.83) and recurrent VTE (HR = 0.80, 95% CI = 0.70-0.91) were lower for apixaban versus warfarin. In this large-scale evaluation of VTE patients receiving outpatient treatment with apixaban or warfarin in U.S. clinical practice, risks of major bleeding, CRNM bleeding and recurrent VTE were significantly lower among patients who received apixaban.
在 AMPLIFY 临床试验中,阿哌沙班在治疗急性静脉血栓栓塞症(VTE)方面不劣于华法林加皮下依诺肝素桥接治疗,且出血风险显著降低。本研究评估了其在常规临床实践中的比较有效性和安全性。采用匹配队列设计和来自美国四个私人医疗保健索赔数据库的数据。研究人群包括在初始 VTE 发作后 30 天内开始门诊接受阿哌沙班与华法林(加静脉用抗凝剂桥接治疗)治疗的患者;阿哌沙班和华法林患者按年龄、VTE 发作特征、研究数据库和倾向评分进行匹配。在 180 天(最长)随访期间,使用共享脆弱性模型比较大出血、临床相关非大出血(CRNM)出血和复发性 VTE。在阿哌沙班患者(n=17878)的平均随访 143 天和华法林患者(n=17878)的平均随访 152 天期间,阿哌沙班与华法林相比,大出血的发生率分别为 1.7%比 2.3%,CRNM 出血分别为 7.0%比 9.4%,复发性 VTE 分别为 2.3%比 2.9%。在共享脆弱性模型中,与华法林相比,阿哌沙班的大出血风险(风险比[HR] = 0.75,95%置信区间[CI] = 0.64-0.87)、CRNM 出血(HR = 0.77,95%CI = 0.71-0.83)和复发性 VTE(HR = 0.80,95%CI = 0.70-0.91)的风险较低。在这项对美国临床实践中接受门诊阿哌沙班或华法林治疗的 VTE 患者的大规模评估中,与接受华法林治疗的患者相比,接受阿哌沙班治疗的患者的大出血、CRNM 出血和复发性 VTE 的风险显著降低。