Ssekubugu Robert, Renju Jenny, Zaba Basia, Seeley Janet, Bukenya Dominic, Ddaaki William, Moshabela Mosa, Wamoyi Joyce, McLean Estelle, Ondenge Kenneth, Skovdal Morten, Wringe Alison
a Rakai Health Sciences Program , Kampala , Uganda.
b Population Studies Group, Faculty of Epidemiology and Public Health , London School of Hygiene and Tropical Medicine, London, UK.
AIDS Care. 2019 Jun;31(6):754-760. doi: 10.1080/09540121.2018.1537467. Epub 2018 Oct 25.
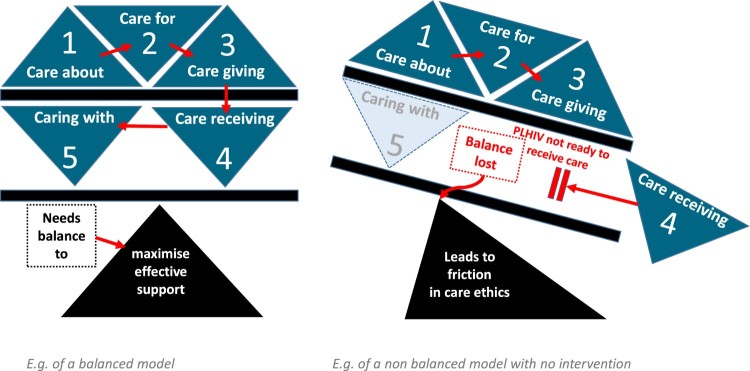
In the era of widespread antiretroviral therapy, few studies have explored the perspectives of the relatives involved in caring for people living with HIV (PLHIV) during periods of ill-health leading up to their demise. In this analysis, we explore the process of care for PLHIV as their death approached, from their relatives' perspective. We apply Tronto's care ethics framework that distinguishes between care-receiving among PLHIV on the one hand, and caring about, caring for and care-giving by their relatives on the other. We draw on 44 in-depth interviews conducted with caregivers following the death of their relatives, in seven rural settings in Eastern and Southern Africa. Relatives suggested that prior to the onset of poor health, few of the deceased had disclosed their HIV status and fewer still were relying on anyone for help. This lack of disclosure meant that some caregivers spoke of enduring a long period of worry, and feelings of helplessness as they were unable to translate their concern and "caring about" into "caring for". This transition often occurred when the deceased became in need of physical, emotional or financial care. The responsibility was often culturally prescribed, rarely questioned and usually fell to women. The move to "care-giving" was characterised by physical acts of providing care for their relative, which lasted until death. Tronto's conceptualisation of caring relationships highlights how the burden of caring often intensifies as family members' caring evolves from "caring about", to "caring for", and eventually to "giving care" to their relatives. This progression can lead to caregivers experiencing frustration, provoking tensions with their relatives and highlighting the need for interventions to support family members caring for PLHIV. Interventions should also encourage PLHIV to disclose their HIV status and seek early access to HIV care and treatment services.
在抗逆转录病毒疗法广泛应用的时代,很少有研究探讨在感染艾滋病毒者(PLHIV)患病直至死亡期间,其亲属在照料过程中的观点。在本分析中,我们从亲属的角度探讨了PLHIV临近死亡时的照料过程。我们应用了特龙托的关怀伦理框架,该框架一方面区分了PLHIV接受照料的情况,另一方面区分了其亲属的关心、照料和给予照料的情况。我们借鉴了在东非和南部非洲七个农村地区对亲属去世后的照料者进行的44次深入访谈。亲属们表示,在健康状况恶化之前,很少有死者透露自己的艾滋病毒感染状况,更少有人依靠他人提供帮助。这种缺乏披露意味着一些照料者表示,他们长期忧心忡忡,感到无助,因为他们无法将自己的关心和“关怀”转化为“照料”。这种转变通常发生在死者需要身体、情感或经济照料之时。责任通常由文化规定,很少受到质疑,而且通常落在女性身上。向“给予照料”的转变以对亲属提供照料的实际行动为特征,这种行动一直持续到亲属去世。特龙托对关怀关系的概念化突出表明,随着家庭成员的关怀从“关心”演变为“照料”,最终变为“给予照料”,照料负担往往会加剧。这种进展可能导致照料者感到沮丧,引发与亲属的紧张关系,并凸显出需要采取干预措施来支持照料PLHIV的家庭成员。干预措施还应鼓励PLHIV披露其艾滋病毒感染状况,并尽早获得艾滋病毒护理和治疗服务。