Departments of Epidemiology.
Health Care Organization and Policy.
Med Care. 2018 Dec;56(12):1051-1059. doi: 10.1097/MLR.0000000000001004.
Assess the validity of Medicare claims for identifying myocardial infarction (MI).
We used data from 9951 Medicare beneficiaries 65 years and above in the Reasons for Geographic And Racial Differences in Stroke study. Between 2003 and 2012, 669 participants had an MI identified and adjudicated through study procedures (ie, the gold standard), and 552 had an overnight inpatient claim with a code for MI (ICD-9 code 410.x0 or 410.x1) in any discharge diagnosis position.
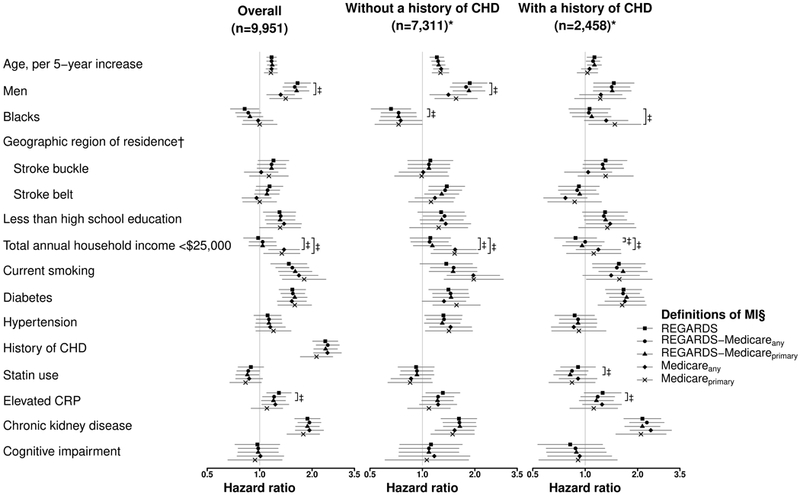
Using Medicare claims with a discharge diagnosis code for MI in any position, the positive predictive value (PPV) was 84.3% [95% confidence interval (CI), 80.9%-87.3%] and the sensitivity was 49.0% (95% CI, 44.9%-53.1%). Sensitivity was lower for men (45.8%) versus women (55.1%), microsize MIs (13.7%) versus other MIs (64.7%), type 2 (30.9%), and 4-5 MIs (11.1%) versus type 1 MIs (76.6%), and MIs occurring in-hospital (28.8%) versus out-of-hospital (66.7%). Using Medicare claims with a code for MI in the primary discharge diagnosis position, the PPV was 89.7% (95% CI, 86.3%-92.5%) and sensitivity was 40.1% (95% CI, 36.1%-44.2%). The sensitivity of claims with a code for MI in the primary discharge diagnosis position was lower for microsize versus other MIs, type 2 and 4-5 MIs versus type 1 MIs and MIs occurring in-hospital versus out-of-hospital. Hazard ratios for MI associated with participant characteristics were similar using adjudicated MIs identified through study procedures or claims for MI without further adjudication.
Medicare claims have a high PPV but low sensitivity for identifying MI and can be used to investigate individual-level characteristics associated with MI.
评估医疗保险索赔在识别心肌梗死(MI)方面的有效性。
我们使用了 Reasons for Geographic And Racial Differences in Stroke 研究中的 9951 名 65 岁及以上的 Medicare 受益人的数据。在 2003 年至 2012 年期间,有 669 名参与者通过研究程序(即黄金标准)确定并裁定发生了 MI,并且有 552 名参与者在任何出院诊断位置的过夜住院索赔中都有 MI 的编码(ICD-9 代码 410.x0 或 410.x1)。
使用医疗保险索赔中任何位置的 MI 出院诊断代码,阳性预测值(PPV)为 84.3%(95%置信区间[CI],80.9%-87.3%),敏感性为 49.0%(95%CI,44.9%-53.1%)。男性(45.8%)的敏感性低于女性(55.1%),微梗死(13.7%)的敏感性低于其他梗死(64.7%),2 型(30.9%)和 4-5 型(11.1%)的敏感性低于 1 型(76.6%),以及住院期间(28.8%)发生的 MI 敏感性高于院外(66.7%)。使用医疗保险索赔中主要出院诊断位置的 MI 编码,PPV 为 89.7%(95%CI,86.3%-92.5%),敏感性为 40.1%(95%CI,36.1%-44.2%)。在主要出院诊断位置的 MI 编码的索赔中,微梗死、2 型和 4-5 型与 1 型 MI 以及住院期间发生的 MI 比院外发生的 MI 的敏感性更低。使用通过研究程序确定的经裁决的 MI 或未经进一步裁决的 MI 索赔来识别 MI 时,与参与者特征相关的 MI 的风险比相似。
医疗保险索赔在识别 MI 方面具有较高的 PPV,但敏感性较低,可以用于调查与 MI 相关的个体特征。