1 Division of Vascular Surgery St. Michael's Hospital Toronto Ontario Canada.
5 Department of Surgery University of Toronto Ontario Canada.
J Am Heart Assoc. 2018 Aug 21;7(16):e009745. doi: 10.1161/JAHA.118.009745.
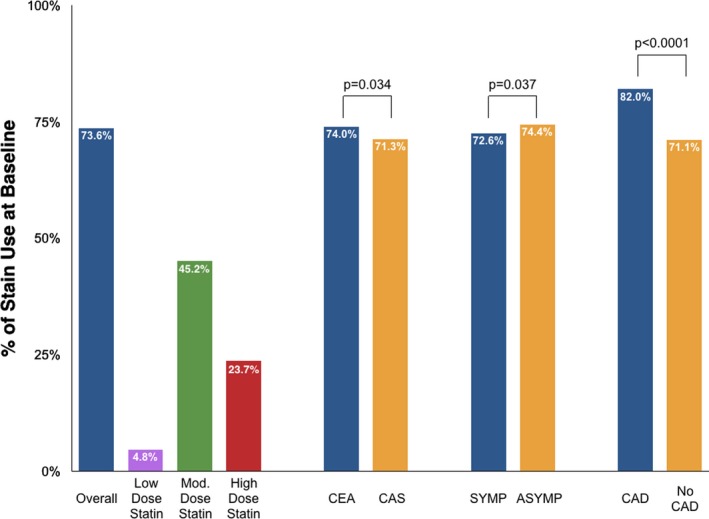
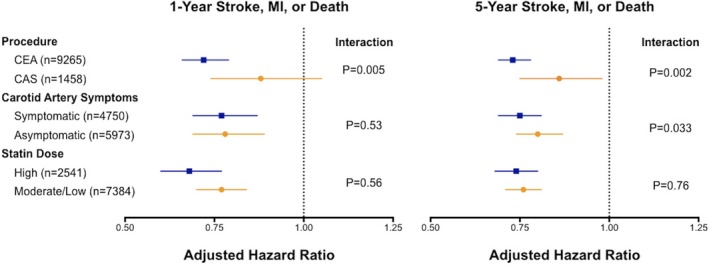
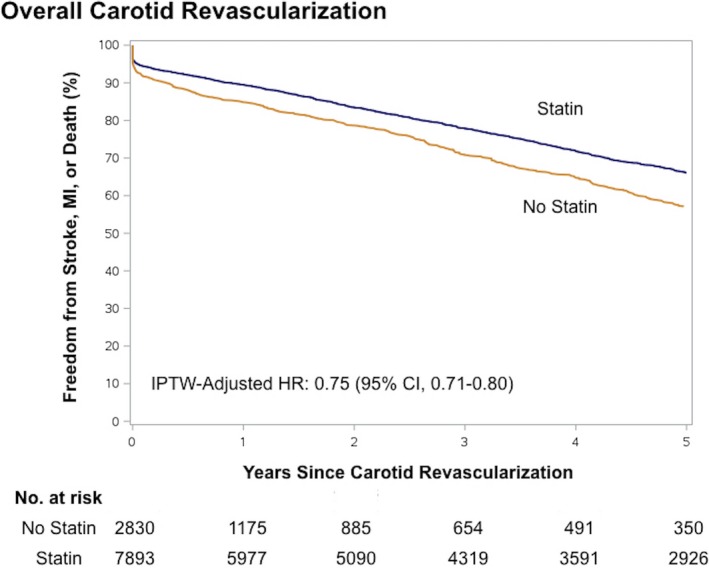
Background Statins are commonly used for the prevention of cardiovascular events; however, statins are underutilized in patients with noncoronary atherosclerosis. We sought to establish the rates of statin use in patients with carotid artery disease and to examine the association between statin therapy and outcomes after carotid revascularization. Methods and Results In this population-level retrospective cohort study, we identified all individuals aged ≥66 years who underwent carotid endarterectomy or stenting in Ontario, Canada (2002-2014). The primary outcome was a composite of 1-year stroke, myocardial infarction, or death (major adverse cardiac and cerebrovascular events). Five-year risks were also examined. Adjusted hazard ratios were computed using inverse probability of treatment weighting based on propensity scores. A total of 7893 of 10 723 patients (73.6%) who underwent carotid revascularization were on preprocedural statin therapy; moderate- or high-dose therapy was utilized by 7384 patients (68.9%). The composite rate of 1-year major adverse cardiac and cerebrovascular events was lower among statin users (adjusted hazard ratio: 0.76; 95% confidence interval, 0.70-0.83). Patients who were on persistent long-term statin therapy after the carotid procedure continued to experience significantly lower risk of major adverse cardiac and cerebrovascular events at 5 years (adjusted hazard ratio: 0.75, 95% confidence interval, 0.71-0.80). The beneficial associations with statin use were observed regardless of type of carotid revascularization procedure, carotid artery symptom status, or statin dose. Conclusions Continuous statin therapy was associated with a 25% lower risk of long-term adverse cardiovascular events in patients with significant carotid disease. Along with other supportive evidence, statins should be considered in patients undergoing carotid revascularization, and efforts are required to increase statin use in this undertreated population.
他汀类药物常用于预防心血管事件;然而,在非冠状动脉粥样硬化患者中,他汀类药物的使用不足。我们旨在确定颈动脉疾病患者使用他汀类药物的比率,并研究他汀类药物治疗与颈动脉血运重建后结局之间的关系。
在这项人群水平的回顾性队列研究中,我们确定了在加拿大安大略省接受颈动脉内膜切除术或支架置入术的所有年龄≥66 岁的个体(2002-2014 年)。主要结局是 1 年内发生卒中、心肌梗死或死亡(主要不良心脏和脑血管事件)的复合结局。还检查了 5 年的风险。使用基于倾向评分的逆概率治疗加权计算调整后的危害比。在接受颈动脉血运重建的 10723 例患者中,共有 7893 例(73.6%)患者术前正在服用他汀类药物;7384 例(68.9%)患者使用了中剂量或高剂量他汀类药物。他汀类药物使用者的 1 年主要不良心脏和脑血管事件复合发生率较低(调整后的危害比:0.76;95%置信区间,0.70-0.83)。在颈动脉手术后持续接受长期他汀类药物治疗的患者,5 年内主要不良心脏和脑血管事件的风险持续显著降低(调整后的危害比:0.75,95%置信区间,0.71-0.80)。无论颈动脉血运重建术的类型、颈动脉症状状态或他汀类药物剂量如何,使用他汀类药物均与他汀类药物使用相关的获益关联。
在患有严重颈动脉疾病的患者中,持续他汀类药物治疗与长期不良心血管事件风险降低 25%相关。结合其他支持性证据,在接受颈动脉血运重建的患者中应考虑使用他汀类药物,并且需要努力增加在这一治疗不足人群中的他汀类药物使用。