Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, ON, Canada.
Programs for Assessment of Technology in Health (PATH), The Research Institute of St. Joe's Hamilton, St. Joseph's Healthcare, Hamilton, ON, Canada.
BMC Geriatr. 2018 Nov 1;18(1):262. doi: 10.1186/s12877-018-0952-7.
Senior high cost health care users (HCU) are a priority for many governments. Little research has addressed regional variation of HCU incidence and outcomes, especially among incident HCU. This study describes the regional variation in healthcare costs and mortality across Ontario's health planning districts [Local Health Integration Networks (LHIN)] among senior incident HCU and non-HCU and explores the relationship between healthcare spending and mortality.
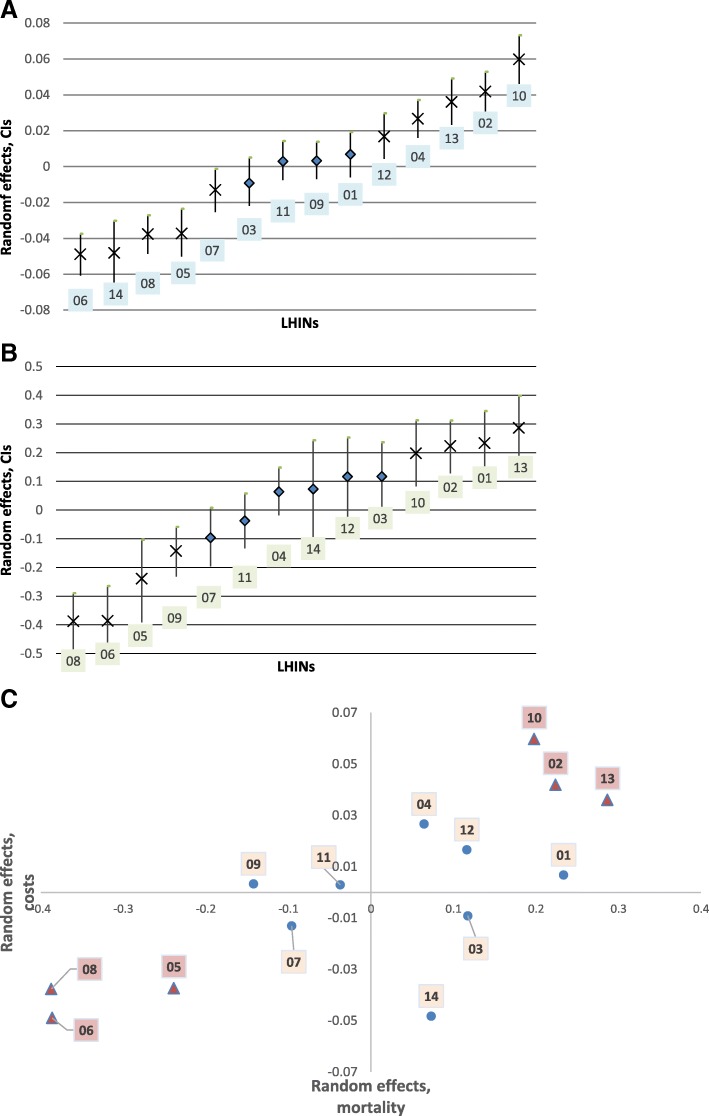
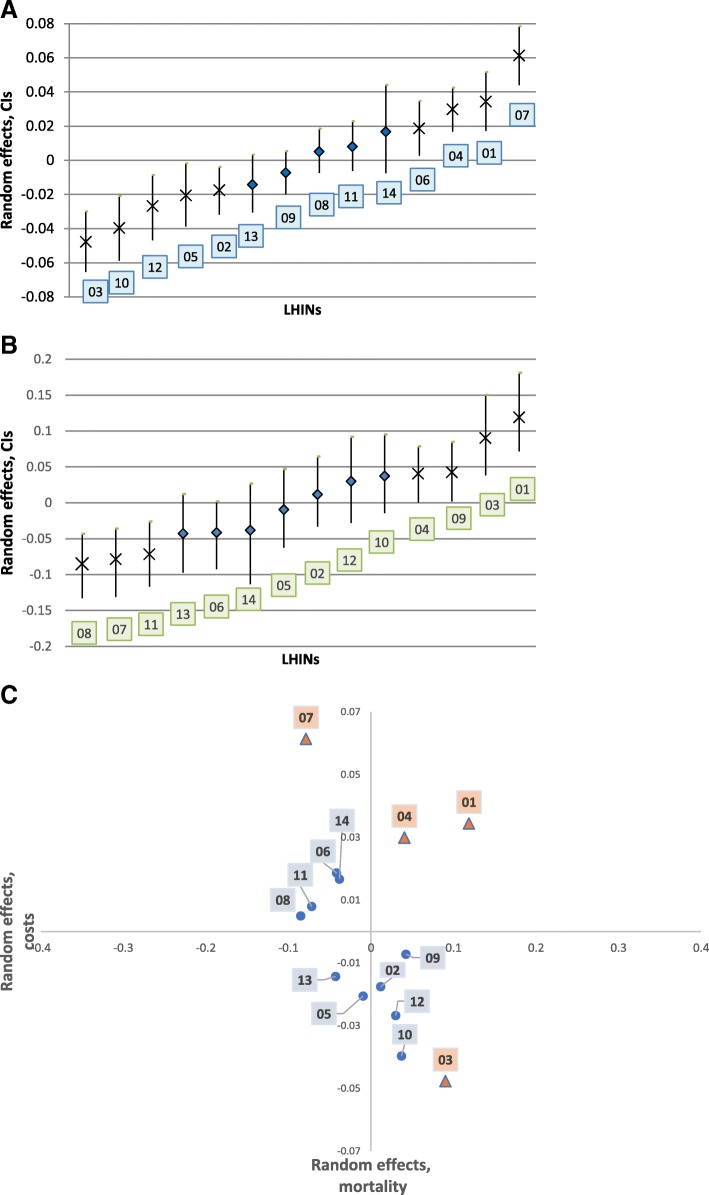
We conducted a retrospective population-based matched cohort study of incident senior HCU defined as Ontarians aged ≥66 years in the top 5% most costly healthcare users in fiscal year (FY) 2013. We matched HCU to non-HCU (1:3) based on age, sex and LHIN. Primary outcomes were LHIN-based variation in costs (total and 12 cost components) and mortality during FY2013 as measured by variance estimates derived from multi-level models. Outcomes were risk-adjusted for age, sex, ADGs, and low-income status. In a cost-mortality analysis by LHIN, risk-adjusted random effects for total costs and mortality were graphically presented together in a cost-mortality plane to identify low and high performers.
We studied 175,847 incident HCU and 527,541 matched non-HCU. On average, 94 out of 1000 seniors per LHIN were HCU (CV = 4.6%). The mean total costs for HCU in FY2013 were 12 times higher that of non-HCU ($29,779 vs. $2472 respectively), whereas all-cause mortality was 13.6 times greater (103.9 vs. 7.5 per 1000 seniors). Regional variation in costs and mortality was lower in senior HCU compared with non-HCU. We identified greater variability in accessing the healthcare system, but, once the patient entered the system, variation in costs was low. The traditional drivers of costs and mortality that we adjusted for played little role in driving the observed variation in HCUs' outcomes. We identified LHINs that had high mortality rates despite elevated healthcare expenditures and those that achieved lower mortality at lower costs. Some LHINs achieved low mortality at excessively high costs.
Risk-adjusted allocation of healthcare resources to seniors in Ontario is overall similar across health districts, more so for HCU than non-HCU. Identified important variation in the cost-mortality relationship across LHINs needs to be further explored.
高成本医疗保健使用者(HCU)是许多政府的优先事项。很少有研究涉及 HCU 发生率和结果的区域差异,尤其是在新发生的 HCU 中。本研究描述了安大略省卫生规划区[地方卫生集成网络(LHIN)]中老年人新发生的 HCU 和非 HCU 的医疗保健成本和死亡率的区域差异,并探讨了医疗保健支出与死亡率之间的关系。
我们对 2013 财年(FY)前 5%的医疗费用最高的老年人中定义的新发生的高级 HCU 进行了回顾性基于人群的匹配队列研究。我们根据年龄、性别和 LHIN 将 HCU 与非 HCU(1:3)匹配。主要结果是 FY2013 基于 LHIN 的成本(总费用和 12 个费用组成部分)和死亡率的变化,通过多水平模型得出的方差估计来衡量。结果根据年龄、性别、ADG 和低收入状况进行风险调整。在按 LHIN 进行的成本-死亡率分析中,总成本和死亡率的风险调整随机效应在成本-死亡率平面上一起以图形方式呈现,以确定低绩效和高绩效者。
我们研究了 175847 名新发生的 HCU 和 527541 名匹配的非 HCU。平均而言,每个 LHIN 中有 94 名老年人是 HCU(变异系数为 4.6%)。2013 财年 HCU 的总费用平均是非 HCU 的 12 倍(分别为 29779 美元和 2472 美元),而全因死亡率高 13.6 倍(每 1000 名老年人中分别为 103.9 人和 7.5 人)。与非 HCU 相比,老年 HCU 的成本和死亡率的区域差异较小。我们发现,在获得医疗保健系统方面的差异较大,但一旦患者进入系统,成本的变化就很小。我们调整的成本和死亡率的传统驱动因素在解释 HCU 结果的变化方面作用不大。我们确定了一些 LHIN,尽管医疗支出较高,但死亡率较高,而一些 LHIN 在降低成本的同时实现了较低的死亡率。一些 LHIN 以过高的成本实现了低死亡率。
安大略省对老年人的医疗保健资源的风险调整分配在整体上在卫生区之间是相似的,对于 HCU 比非 HCU 更为相似。需要进一步探讨在 LHIN 之间发现的与成本-死亡率关系有关的重要差异。