Institut NuMeCan, Université de Rennes 1, Institut national de la recherche agronomique (INRA), Institut national de la santé et de la recherche médicale (INSERM), Rennes F-35000, France.
Department of Pathology, Department of Medicine (Gastroenterology and Hepatology), University of Illinois at Chicago, IL 60612, United States.
World J Gastroenterol. 2018 Oct 28;24(40):4536-4547. doi: 10.3748/wjg.v24.i40.4536.
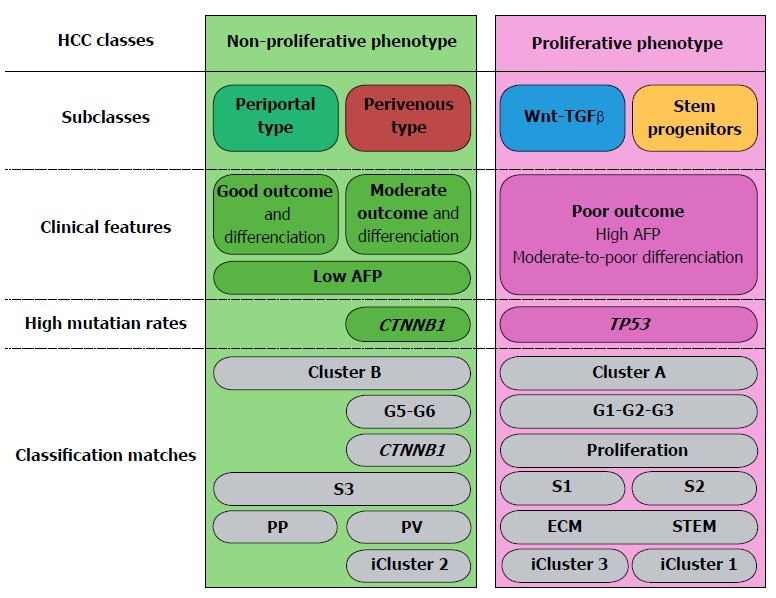
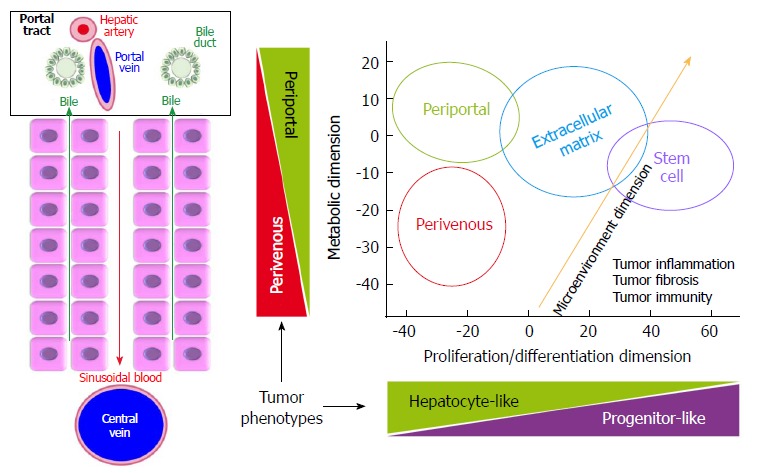
Hepatocellular carcinoma (HCC) is the 3 leading cause of cancer-related death worldwide. More than 80% of HCCs arise within chronic liver disease resulting from viral hepatitis, alcohol, hemochromatosis, obesity and metabolic syndrome or genotoxins. Projections based on Western lifestyle and its metabolic consequences anticipate a further increase in incidence, despite recent breakthroughs in the management of viral hepatitis. HCCs display high heterogeneity of molecular phenotypes, which challenges clinical management. However, emerging molecular classifications of HCCs have not yet formed a unified corpus translatable to the clinical practice. Thus, patient management is currently based upon tumor number, size, vascular invasion, performance status and functional liver reserve. Nonetheless, an impressive body of molecular evidence emerged within the last 20 years and is becoming increasingly available to medical practitioners and researchers in the form of repositories. Therefore, the aim this work is to review molecular data underlying HCC classifications and to organize this corpus into the major dimensions explaining HCC phenotypic diversity. Major efforts have been recently made worldwide toward a unifying "clinically-friendly" molecular landscape. As a result, a consensus emerges on three major dimensions explaining the HCC heterogeneity. In the first dimension, tumor cell proliferation and differentiation enabled allocation of HCCs to two major classes presenting profoundly different clinical aggressiveness. In the second dimension, HCC microenvironment and tumor immunity underlie recent therapeutic breakthroughs prolonging patients' survival. In the third dimension, metabolic reprogramming, with the recent emergence of subclass-specific metabolic profiles, may lead to adaptive and combined therapeutic approaches. Therefore, here we review recent molecular evidence, their impact on tumor histopathological features and clinical behavior and highlight the remaining challenges to translate our cognitive corpus into patient diagnosis and allocation to therapeutic options.
肝细胞癌 (HCC) 是全球癌症相关死亡的第 3 大原因。超过 80%的 HCC 发生在由病毒性肝炎、酒精、血色病、肥胖和代谢综合征或遗传毒素引起的慢性肝病中。尽管最近在病毒性肝炎的治疗方面取得了突破,但基于西方生活方式及其代谢后果的预测表明,发病率还会进一步上升。HCC 的分子表型具有高度异质性,这给临床管理带来了挑战。然而,新兴的 HCC 分子分类尚未形成可转化为临床实践的统一体系。因此,目前患者的管理主要基于肿瘤数量、大小、血管侵犯、身体状况和肝功能储备。尽管如此,在过去的 20 年中,大量的分子证据已经出现,并以存储库的形式越来越多地提供给医疗从业者和研究人员。因此,本研究旨在回顾 HCC 分类的分子数据,并将该体系组织成主要维度,以解释 HCC 表型多样性。最近,全球范围内在实现统一的“临床友好”分子图谱方面做出了巨大努力。结果,在三个主要维度上达成了共识,这些维度解释了 HCC 的异质性。在第一个维度中,肿瘤细胞的增殖和分化使 HCC 分为两类,这两类 HCC 的临床侵袭性明显不同。在第二个维度中,HCC 微环境和肿瘤免疫是最近治疗突破的基础,这些突破延长了患者的生存时间。在第三个维度中,代谢重编程,以及最近出现的特定亚类的代谢特征,可能导致适应性和联合治疗方法。因此,我们在这里回顾了最近的分子证据,及其对肿瘤组织病理学特征和临床行为的影响,并强调了将我们的认知体系转化为患者诊断和治疗选择的挑战。