Department of Renal Medicine, University Hospital Geelong, Rotary House, 325 Ryrie St, Geelong, VIC, Australia.
IMPACT Strategic Research Centre, School of Medicine, Barwon Health, Deakin University, 75 Pigdons Road, Geelong, Australia.
BMC Nephrol. 2018 Nov 3;19(1):305. doi: 10.1186/s12882-018-1101-4.
Despite lithium being the most efficacious treatment for bipolar disorder, its use has been decreasing at least in part due to concerns about its potential to cause significant nephrotoxicity. Whilst the ability of lithium to cause nephrogenic diabetes insipidus is well established, its ability to cause chronic kidney disease is a much more vexing issue, with various studies suggesting both positive and negative causality. Despite these differences, the weight of evidence suggests that lithium has the potential to cause end stage kidney disease, albeit over a prolonged period.
A search strategy for this review was developed to identify appropriate studies, sourced from the electronic databases EMBASE, PubMed (NLM) and MEDLINE. Search terms included lithium with the AND operator to combine with nephrotoxicity or nephropathy or chronic kidney disease or nephrogenic diabetes insipidus or renal and pathophysiology.
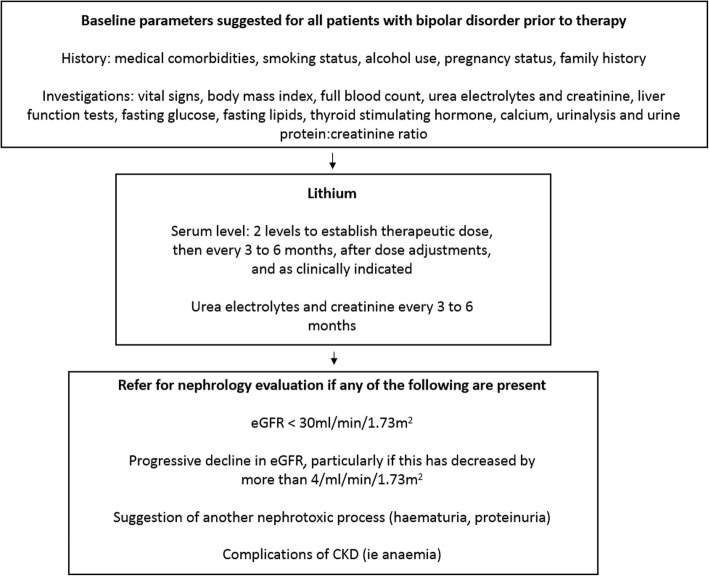
The risks for the development of lithium induced nephropathy are less well defined but appear to include the length of duration of therapy as well as increasing age, as well as episodes of over dosage/elevated lithium levels. Whilst guidelines exist for the routine monitoring of lithium levels and renal function, it remains unclear when nephrological evaluation should occur, as well as when cessation of lithium therapy is appropriate balancing the significant attendant mental health risks as well as the potential for progression to occur despite cessation of therapy against the risks and morbidity of bipolar disorder itself.
This paper will elucidate on the current evidence pertaining to the topic of the clinical management of lithium induced nephrotoxicity and provide a guide for clinicians who are faced with the long-term management of these patients.
尽管锂是治疗双相情感障碍最有效的药物,但由于担心其可能导致严重的肾毒性,其使用至少在一定程度上有所减少。虽然锂引起肾性尿崩症的能力已得到充分证实,但它引起慢性肾脏病的能力则是一个更加棘手的问题,各种研究表明存在正反两方面的因果关系。尽管存在这些差异,但大量证据表明,锂有可能导致终末期肾病,尽管这需要一个漫长的过程。
为了确定适当的研究,我们制定了搜索策略,从电子数据库 EMBASE、PubMed(NLM)和 MEDLINE 中获取相关信息。搜索词包括锂,用 AND 运算符将其与肾毒性、肾病、慢性肾脏病、肾性尿崩症或肾脏和病理生理学相结合。
锂诱导的肾病的发展风险不太明确,但似乎包括治疗时间的长短、年龄的增长、以及过量/升高的锂水平发作。虽然存在常规监测锂水平和肾功能的指南,但仍不清楚何时应进行肾病学评估,以及何时停止锂治疗更为合适,既要权衡停止治疗后可能出现的严重精神健康风险,又要权衡继续治疗与双相情感障碍本身的风险和发病率之间的平衡。
本文将阐明关于锂诱导的肾毒性临床管理的当前证据,并为面临这些患者长期管理的临床医生提供指导。