Clinical Research Department, International Centre for Eye Health, London School of Hygiene and Tropical Medicine, Keppel Street, London, WC1E 7HT, UK.
School of Medicine, Dentistry and Biomedical Sciences, Queen's University, 97, Lisburn Road, Belfast, BT9 7BL, Northern Ireland.
Syst Rev. 2018 Nov 7;7(1):182. doi: 10.1186/s13643-018-0846-y.
Visual impairment from diabetic retinopathy (DR) is an increasing global public health concern, which is preventable with screening and early treatment. Digital retinal imaging has become a preferred choice as it enables higher coverage of screening. The aim of this review is to evaluate how different characteristics of the DR screening (DRS) test impact on diagnostic test accuracy (DTA) and its relevance to a low-income setting.
We conducted a systematic literature search to identify clinic-based studies on DRS using digital retinal imaging of people with DM (PwDM). Summary estimates of different sub-groups were calculated using DTA values weighted according to the sample size. The DTA of each screening method was derived after exclusion of ungradable images and considering the eye as the unit of analysis. The meta-analysis included studies which measured DTA of detecting any level of DR. We also examined the effect on detection from using different combinations of retinal fields, pupil status, index test graders and setting.
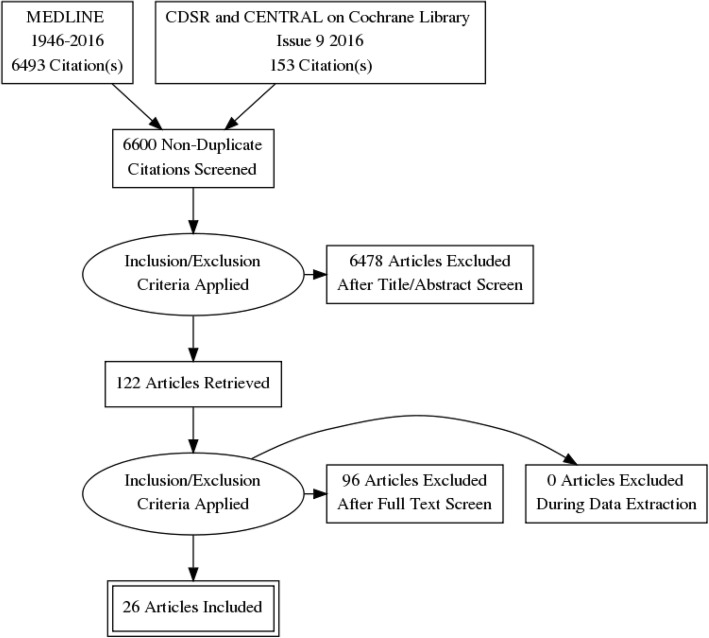
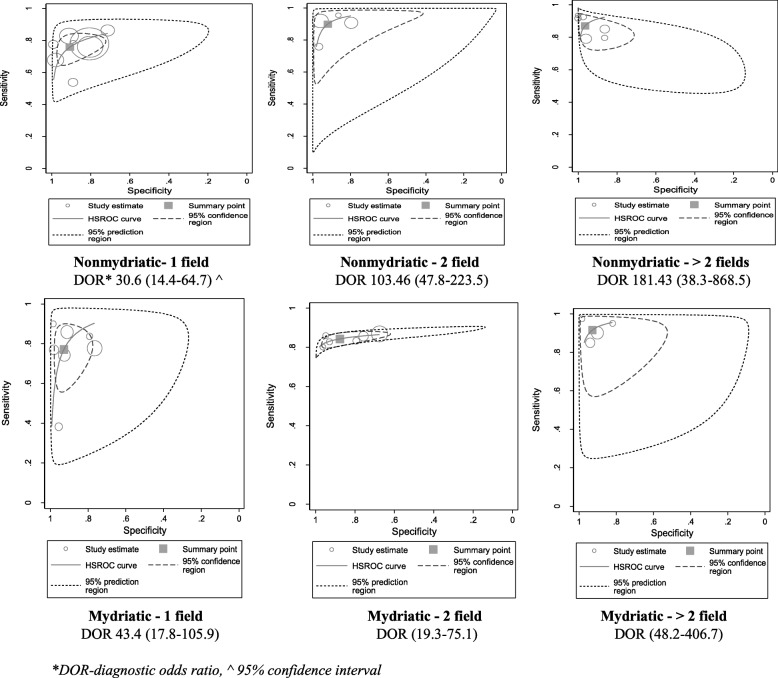
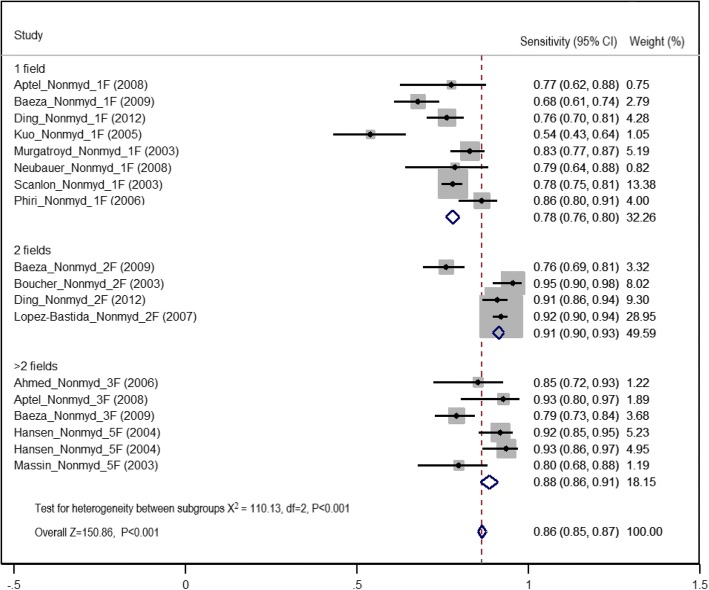
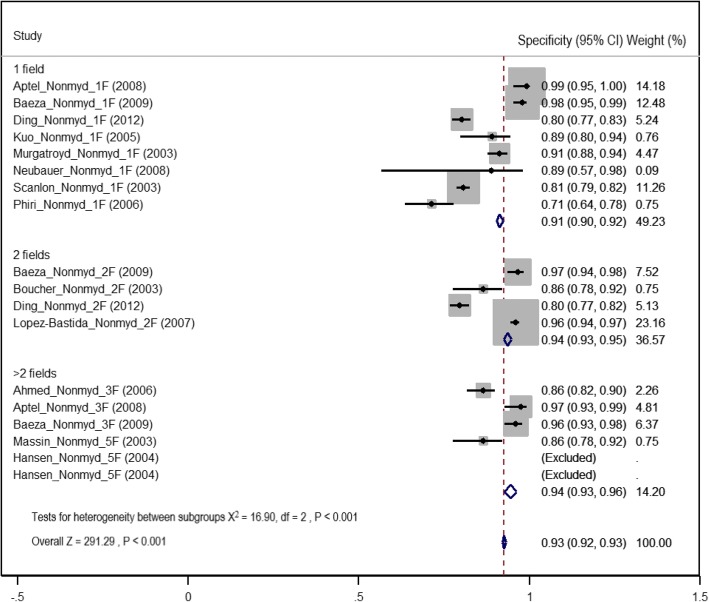
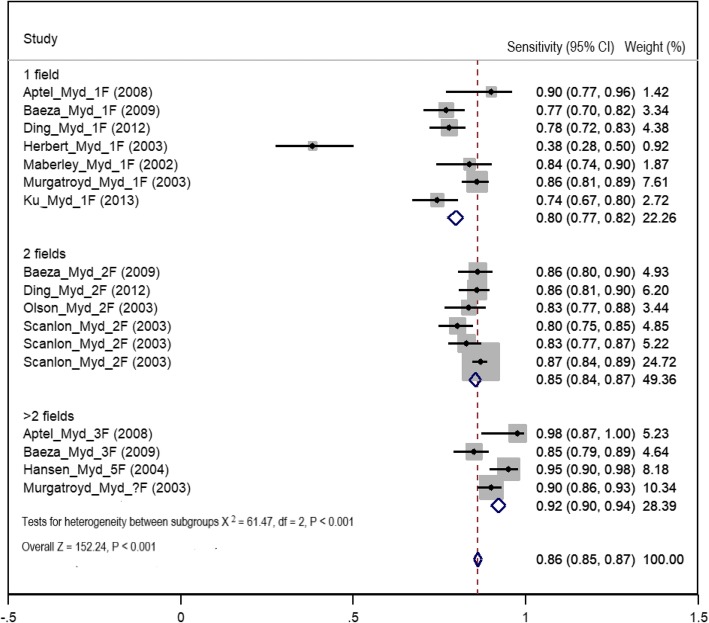
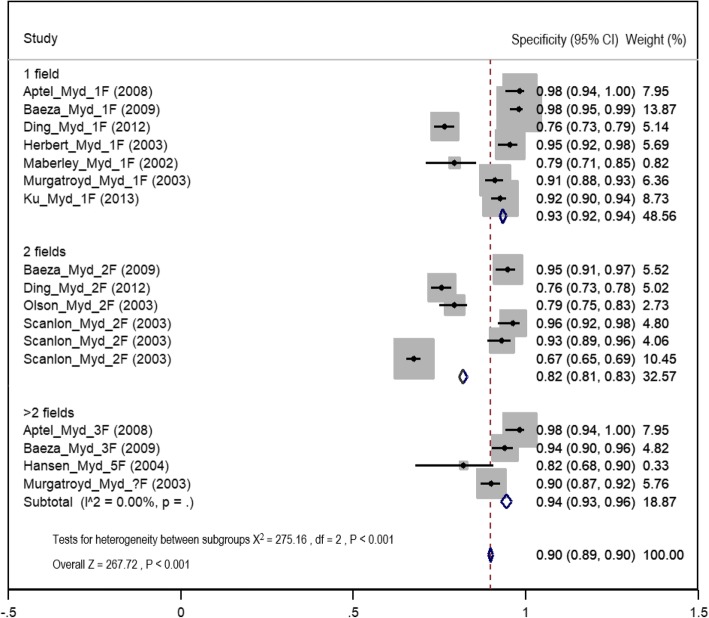
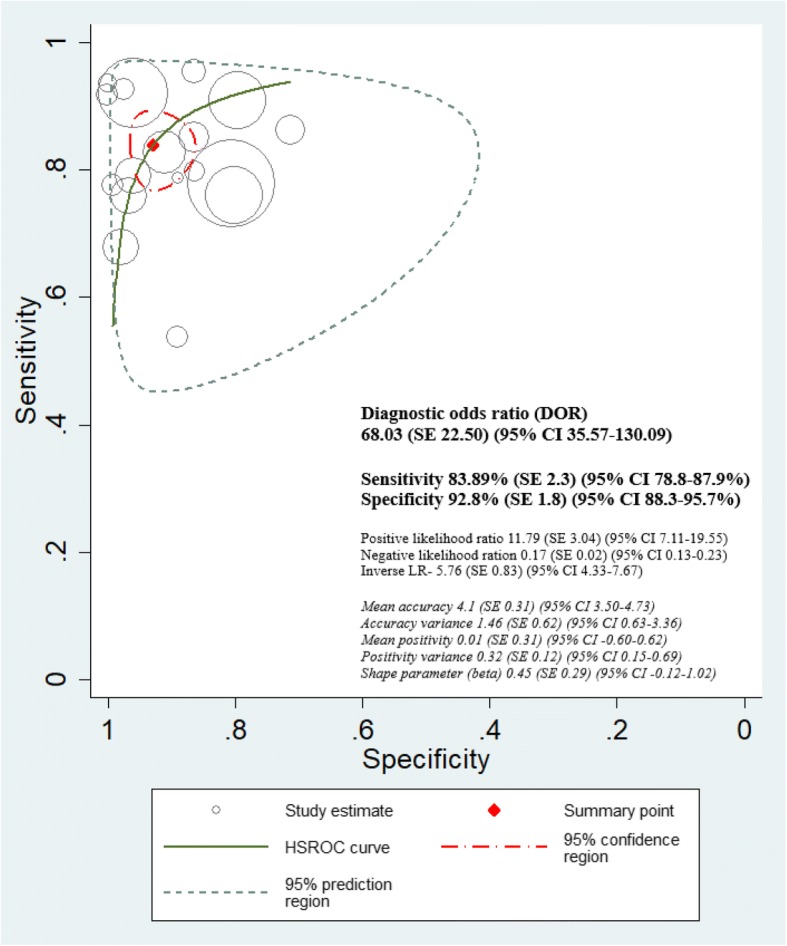
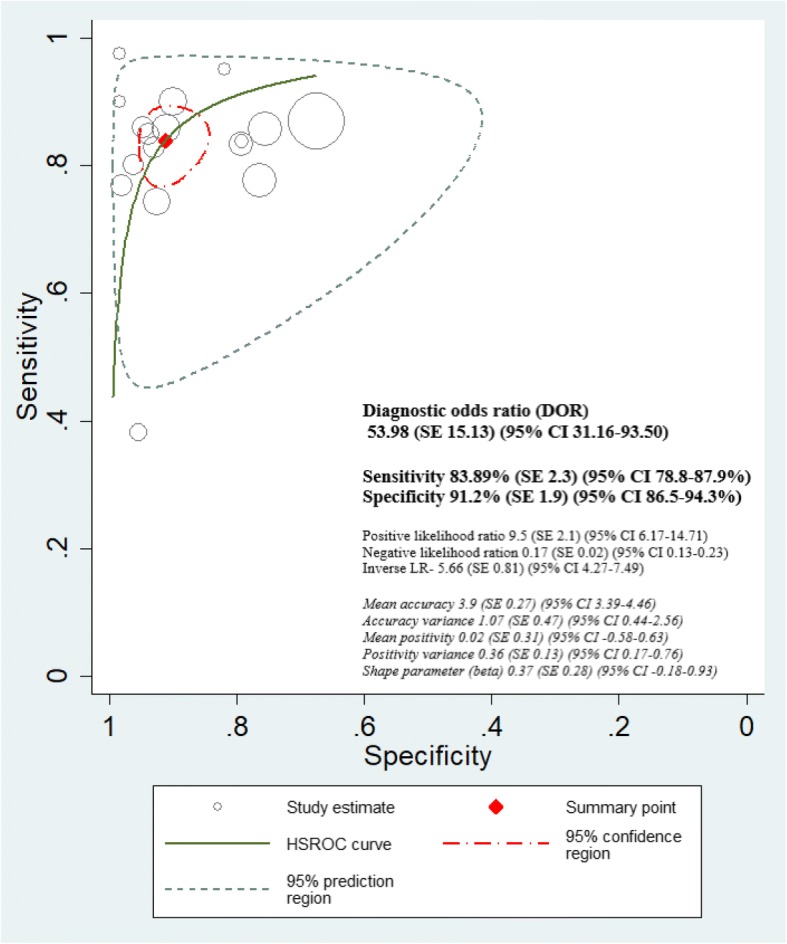
Six thousand six hundred forty-six titles and abstracts were retrieved, and data were extracted from 122 potentially eligible full reports. Twenty-six studies were included in the review, and 21 studies, mostly from high-income settings (18/21, 85.7%), were included in the meta-analysis. The highest sensitivity was observed in the mydriatic greater than two field strategy (92%, 95% CI 90-94%). The highest specificity was observed in greater than two field methods (94%, 95% CI 93-96%) where mydriasis did not affect specificity. Overall, there was no difference in sensitivity between non-mydriatic and mydriatic methods (86%, 95% CI 85-87) after exclusion of ungradable images. The highest DTA (sensitivity 90%, 95% CI 88-91%; specificity 95%, 95% CI 94-96%) was observed when screening was delivered at secondary/tertiary level clinics.
Non-mydriatic two-field strategy could be a more pragmatic approach in starting DRS programmes for facility-based PwDM in low-income settings, with dilatation of the pupils of those who have ungradable images. There was insufficient evidence in primary studies to draw firm conclusions on how graders' background influences DTA. Conducting more context-specific DRS validation studies in low-income and non-ophthalmic settings can be recommended.
糖尿病视网膜病变(DR)导致的视力障碍是一个日益严重的全球公共卫生问题,可以通过筛查和早期治疗来预防。数字视网膜成像已成为首选方法,因为它可以提高筛查的覆盖率。本研究旨在评估 DR 筛查(DRS)测试的不同特征如何影响诊断测试准确性(DTA)及其与低收入环境的相关性。
我们进行了系统的文献检索,以确定使用数字视网膜成像对 DM 患者(PwDM)进行的基于诊所的 DRS 研究。根据样本量对不同亚组的汇总估计值进行加权计算。排除不可分级图像并将眼睛作为分析单位后,得出每种筛查方法的 DTA。荟萃分析包括测量任何程度的 DR 检测的 DTA 的研究。我们还检查了使用不同的视网膜区域组合、瞳孔状态、索引测试分级和设置对检测的影响。
检索到 6646 个标题和摘要,从 122 篇潜在合格的全文报告中提取了数据。综述包括 26 项研究,21 项研究(85.7%来自高收入环境)纳入荟萃分析。散瞳大于两视野策略观察到最高的敏感性(92%,95%CI 90-94%)。大于两视野方法观察到最高的特异性(94%,95%CI 93-96%),散瞳对特异性没有影响。总体而言,排除不可分级图像后,非散瞳和散瞳方法之间的敏感性无差异(86%,95%CI 85-87%)。在二级/三级诊所进行筛查时,观察到最高的 DTA(敏感性 90%,95%CI 88-91%;特异性 95%,95%CI 94-96%)。
在低收入环境中为基于医疗机构的 PwDM 启动 DRS 计划时,非散瞳两视野策略可能是一种更实用的方法,可以对那些不可分级图像的患者进行瞳孔扩张。初级研究中没有足够的证据来得出关于分级员背景如何影响 DTA 的明确结论。可以建议在低收入和非眼科环境中进行更多特定于背景的 DRS 验证研究。