Bowers Riley D, Cooper April A, Wente Catherine L, Wilson Dustin T, Johnson Steven W, Drew Richard H
Department of Pharmacy Practice, College of Pharmacy & Health Sciences, Campbell University. Buies Creek, NC; & Cape Fear Valley Medical Center. Fayetteville, NC (United States).
Department of Pharmacy Practice, College of Pharmacy & Health Sciences, Campbell University. Buies Creek, NC; & Duke Regional Hospital. Durham, NC (United States).
Pharm Pract (Granada). 2018 Jul-Sep;16(3):1204. doi: 10.18549/PharmPract.2018.03.1204. Epub 2018 Aug 13.
There remains variability in both practice and evidence related to optimal initial empiric dosing strategies for vancomycin.
Our primary objective was to describe the percentage of obese patients receiving vancomycin doses consistent with nomogram recommendations achieving targeted initial steady-state serum vancomycin concentrations. Secondary objectives were to describe the primary endpoint in subgroups based on patient weight and estimated creatinine clearance, to describe the rate of supratherapeutic vancomycin accumulation following an initial therapeutic trough concentration, and to describe the rate of vancomycin-related adverse events.
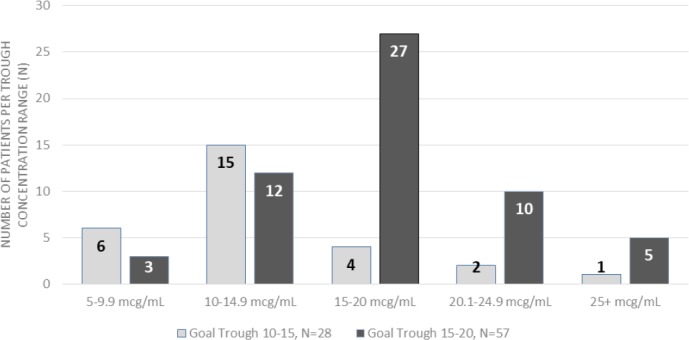
This single-center, IRB-approved, retrospective cohort included adult patients ≥ 100 kilograms total body weight with a body mass index (BMI) >30 kilograms/m2 who received a stable nomogram-based vancomycin regimen and had at least one steady-state vancomycin trough concentration. Data collected included vancomycin regimens and concentrations, vancomycin indication, serum creatinine, and vancomycin-related adverse events. Patients were divided into two cohorts by goal trough concentration: 10-15 mcg/mL and 15-20 mcg/mL.
Of 325 patients screened, 85 were included. Goal steady-state concentrations were reached in 42/85 (49.4%) of total patients.
Achievement of initial steady-state vancomycin serum concentrations in the present study (approximately 50%) was consistent with the use of published vancomycin dosing nomograms.
关于万古霉素最佳初始经验性给药策略,实践和证据仍存在差异。
我们的主要目标是描述接受符合列线图建议剂量万古霉素的肥胖患者中,达到目标初始稳态血清万古霉素浓度的百分比。次要目标是根据患者体重和估计的肌酐清除率描述亚组中的主要终点,描述初始治疗谷浓度后万古霉素超治疗浓度积累的发生率,以及描述万古霉素相关不良事件的发生率。
这项经机构审查委员会批准的单中心回顾性队列研究纳入了体重指数(BMI)>30千克/平方米、总体重≥100千克的成年患者,这些患者接受了基于稳定列线图的万古霉素治疗方案,且至少有一次稳态万古霉素谷浓度。收集的数据包括万古霉素治疗方案和浓度、万古霉素适应证、血清肌酐以及万古霉素相关不良事件。根据目标谷浓度将患者分为两个队列:10 - 15微克/毫升和15 - 20微克/毫升。
在325名筛查患者中,85名被纳入。42/85(49.4%)的患者达到了目标稳态浓度。
本研究中初始稳态万古霉素血清浓度的达成率(约50%)与已发表的万古霉素给药列线图的使用情况一致。