Saad Fady Samy, El Baradie Samia Yehia, Abdel Aliem Maha Abdel Wahab, Ali Mohamed Metwally, Kotb Tamer Ahmed Mahmoud
Department of Anesthesia and Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt.
Saudi J Anaesth. 2018 Oct-Dec;12(4):565-570. doi: 10.4103/sja.SJA_153_18.
Thoracotomy needs adequate powerful postoperative analgesia. This study aims to compare the safety and efficacy of ultrasound (US)-guided serratus anterior plane block (SAPB) and thoracic paravertebral block (TPVB) for perioperative analgesia in cancer patients having lung lobectomy.
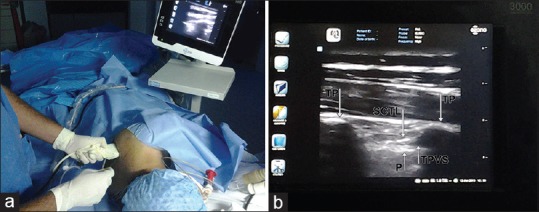
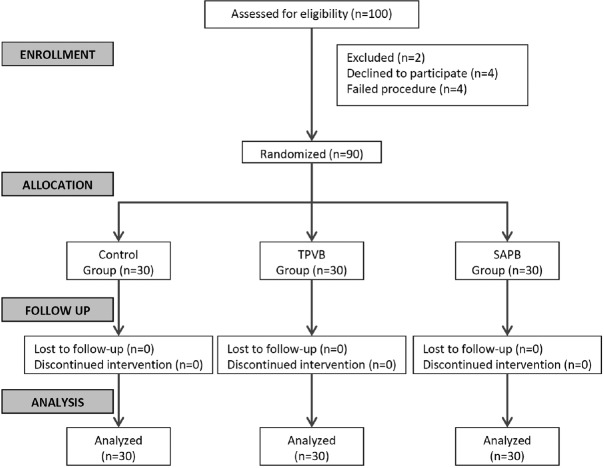
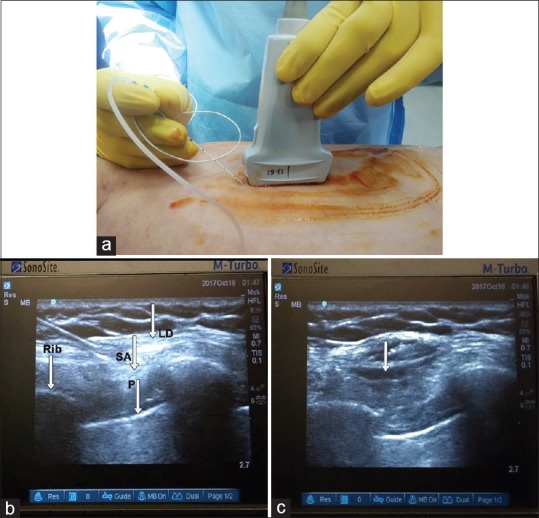
This clinical trial involved 90 patients with lung cancer scheduled for lung lobectomy randomly divided into three groups according to the type of preemptive regional block. Group TPVB received US-guided TPVB. In Group SAPB, US-guided SAPB was performed. The patients of the control Group received general anesthesia alone. The outcome measures were postoperative visual analog scale (VAS) score, intraoperative fentanyl consumption, time of first rescue analgesic, total dose postoperative analgesic, and drug-related adverse effects.
Analgesia was adequate in TPVB and SAPB groups up to 24 h. VAS score was comparable in TPVB and SAPB groups and significantly lower compared to control group up to 9 h postoperatively. At 12 and 24 h, TPVB group had significantly lower VAS score relative to SAPB and control groups. Total intraoperative fentanyl consumption was significantly lower in TPVB and SAPB Groups compared to control group. The majority of TPVB Group cases did not need rescue morphine, while the majority of control group needed two doses ( < 0.001). The hemodynamic variables were stable in all patients. Few cases reported trivial adverse effects.
Preemptive TPVB and SAPB provide comparable levels of adequate analgesia for the first 24 h after thoracotomy. TPVB provided better analgesia after 12 h. The two procedures reduce intraoperative fentanyl and postoperative morphine consumption.
开胸手术需要充分有效的术后镇痛。本研究旨在比较超声(US)引导下前锯肌平面阻滞(SAPB)和胸椎旁神经阻滞(TPVB)用于肺癌肺叶切除术患者围手术期镇痛的安全性和有效性。
本临床试验纳入90例计划行肺叶切除术的肺癌患者,根据预防性区域阻滞类型随机分为三组。TPVB组接受US引导下的TPVB。SAPB组进行US引导下的SAPB。对照组患者仅接受全身麻醉。观察指标包括术后视觉模拟评分(VAS)、术中芬太尼用量、首次补救镇痛时间、术后镇痛总剂量以及药物相关不良反应。
TPVB组和SAPB组在术后24小时内镇痛效果良好。TPVB组和SAPB组的VAS评分相当,术后9小时内显著低于对照组。在术后12小时和24小时,TPVB组的VAS评分相对于SAPB组和对照组显著更低。TPVB组和SAPB组术中芬太尼总用量显著低于对照组。TPVB组大多数病例不需要补救吗啡,而对照组大多数病例需要两剂(<0.001)。所有患者的血流动力学变量均稳定。少数病例报告有轻微不良反应。
预防性TPVB和SAPB在开胸术后的前24小时提供相当水平的充分镇痛。TPVB在术后12小时后提供更好的镇痛效果。这两种方法减少了术中芬太尼和术后吗啡的用量。