Arora Suman, Ovung Ronithung, Bharti Neerja, Yaddanapudi Sandhya, Singh Gurpreet
Post Graduate Institute of Medical Education & Research (PGIMER), Department of Anaesthesia and Intensive Care, Chandigarh, India.
Post Graduate Institute of Medical Education & Research (PGIMER), Department of Anaesthesia and Intensive Care, Chandigarh, India.
Braz J Anesthesiol. 2022 Sep-Oct;72(5):587-592. doi: 10.1016/j.bjane.2021.09.017. Epub 2021 Oct 7.
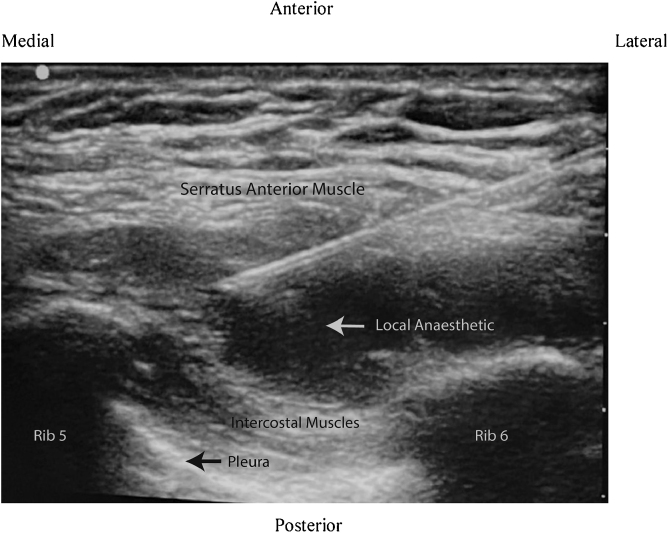
Breast cancer surgery is associated with considerable acute post-surgical pain and restricted mobility. Various regional and neuraxial anesthesia techniques have been used to alleviate post-mastectomy pain. Ultrasound-guided serratus anterior plane block (SAPB) has been considered a simple and safe technique. This randomized control study was performed to compare the efficacy of SAPB with the thoracic paravertebral block (TPVB) for postoperative analgesia after breast cancer surgery.
A total of 40 adult ASA physical status I - II female patients undergoing radical mastectomy were randomly allocated into two groups to receive either ultrasound-guided TPVB or SAPB with 0.4 mL.kg 0.5% ropivacaine, 30 min before surgery. All patients received standardized general anesthesia for surgery. Injection diclofenac and tramadol were used for postoperative rescue analgesia. The time to first rescue analgesia, total analgesic consumption in the first 24 hours, postoperative pain scores, and any adverse effects were recorded.
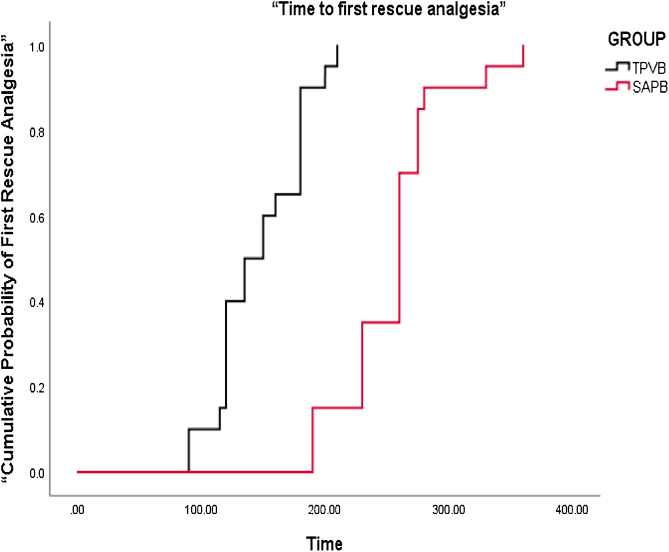
The time to first rescue analgesia was significantly longer in the SAPB group (255.3 ± 47.8 min) as compared with the TPVB group (146.8 ± 30.4 min) (p < 0.001). Total diclofenac consumption in 24 hours was also less in the SAPB group (138.8 ± 44.0 mg vs 210.0 ± 39.2 mg in SAPB and TPVB group respectively, p < 0.001). Postoperative pain scores were significantly lower in the SAPB group as compared with TPVB group (p < 0.05). The incidence of PONV was also less in the SAPB group (p = 0.028). No block-related adverse effects were reported.
We found that the serratus anterior plane block was more effective than the thoracic paravertebral block for postoperative analgesia after breast cancer surgery.
乳腺癌手术会导致相当程度的术后急性疼痛和活动受限。多种区域和神经轴麻醉技术已被用于减轻乳房切除术后疼痛。超声引导下前锯肌平面阻滞(SAPB)被认为是一种简单且安全的技术。本随机对照研究旨在比较SAPB与胸椎旁神经阻滞(TPVB)在乳腺癌手术后镇痛的效果。
总共40例接受根治性乳房切除术的成年ASA身体状况I-II级女性患者被随机分为两组,在手术前30分钟分别接受超声引导下的TPVB或用0.4 mL·kg的0.5%罗哌卡因进行SAPB。所有患者均接受标准化的全身麻醉进行手术。使用双氯芬酸注射液和曲马多进行术后补救镇痛。记录首次补救镇痛的时间、前24小时的总镇痛药物消耗量、术后疼痛评分以及任何不良反应。
与TPVB组(146.8±30.4分钟)相比,SAPB组首次补救镇痛的时间显著更长(255.3±±47.8分钟)(p<0.001)。SAPB组24小时内双氯芬酸的总消耗量也更少(分别为138.8±44.0毫克和210.0±39.2毫克,p<0.001)。与TPVB组相比,SAPB组术后疼痛评分显著更低(p<0.05)。SAPB组恶心呕吐的发生率也更低(p=0.028)。未报告与阻滞相关的不良反应。
我们发现前锯肌平面阻滞在乳腺癌手术后镇痛方面比胸椎旁神经阻滞更有效。