Department of Anesthesiology and Critical Care Medicine, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.
Division of Cardiology, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.
Catheter Cardiovasc Interv. 2019 Feb 15;93(3):E143-E152. doi: 10.1002/ccd.27962. Epub 2018 Nov 15.
Pulmonary insufficiency is a consequence of transannular patch repair in Tetralogy of Fallot (ToF) leading to late morbidity and mortality. Transcatheter native outflow tract pulmonary valve replacement has become a reality. However, predicting a secure, atraumatic implantation of a catheter-based device remains a significant challenge due to the complex and dynamic nature of the right ventricular outflow tract (RVOT). We sought to quantify the differences in compression and volume for actual implants, and those predicted by pre-implant modeling.
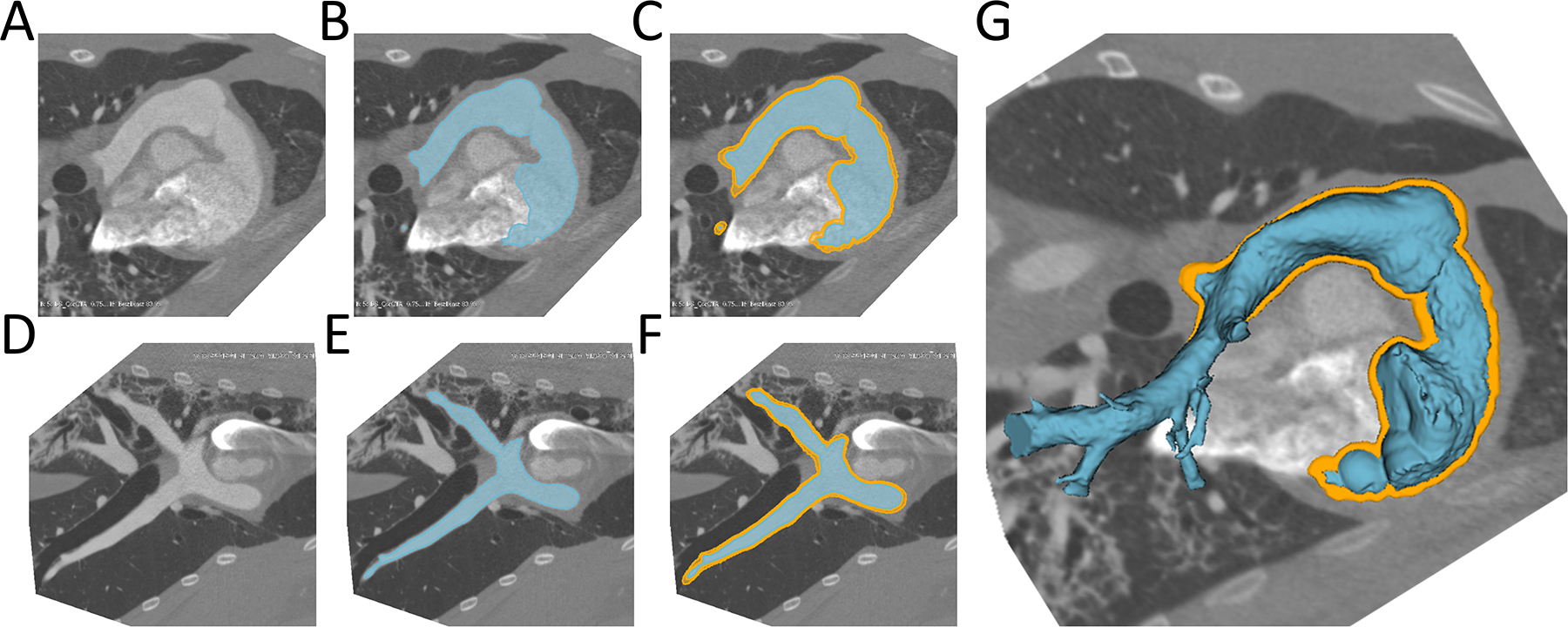
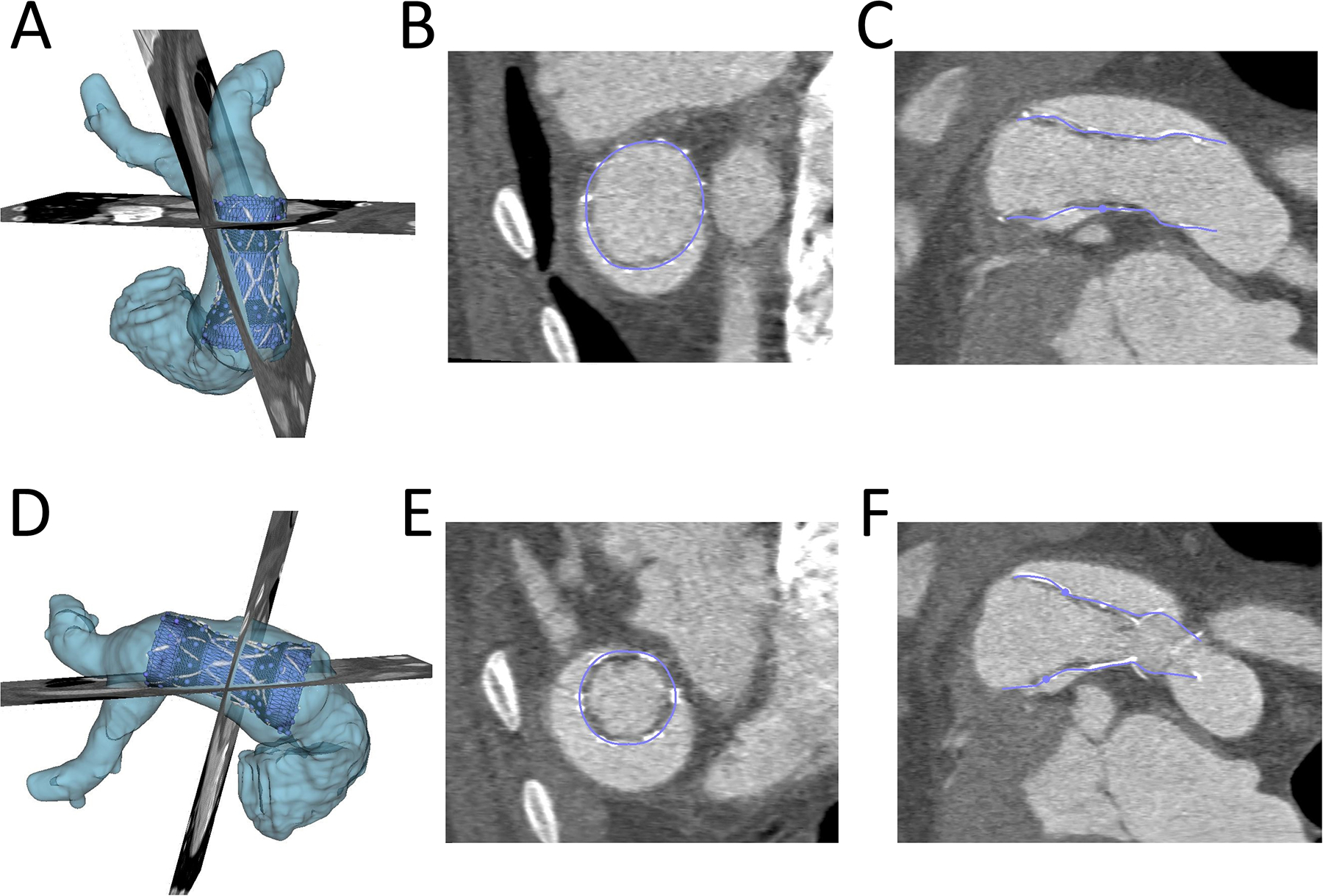
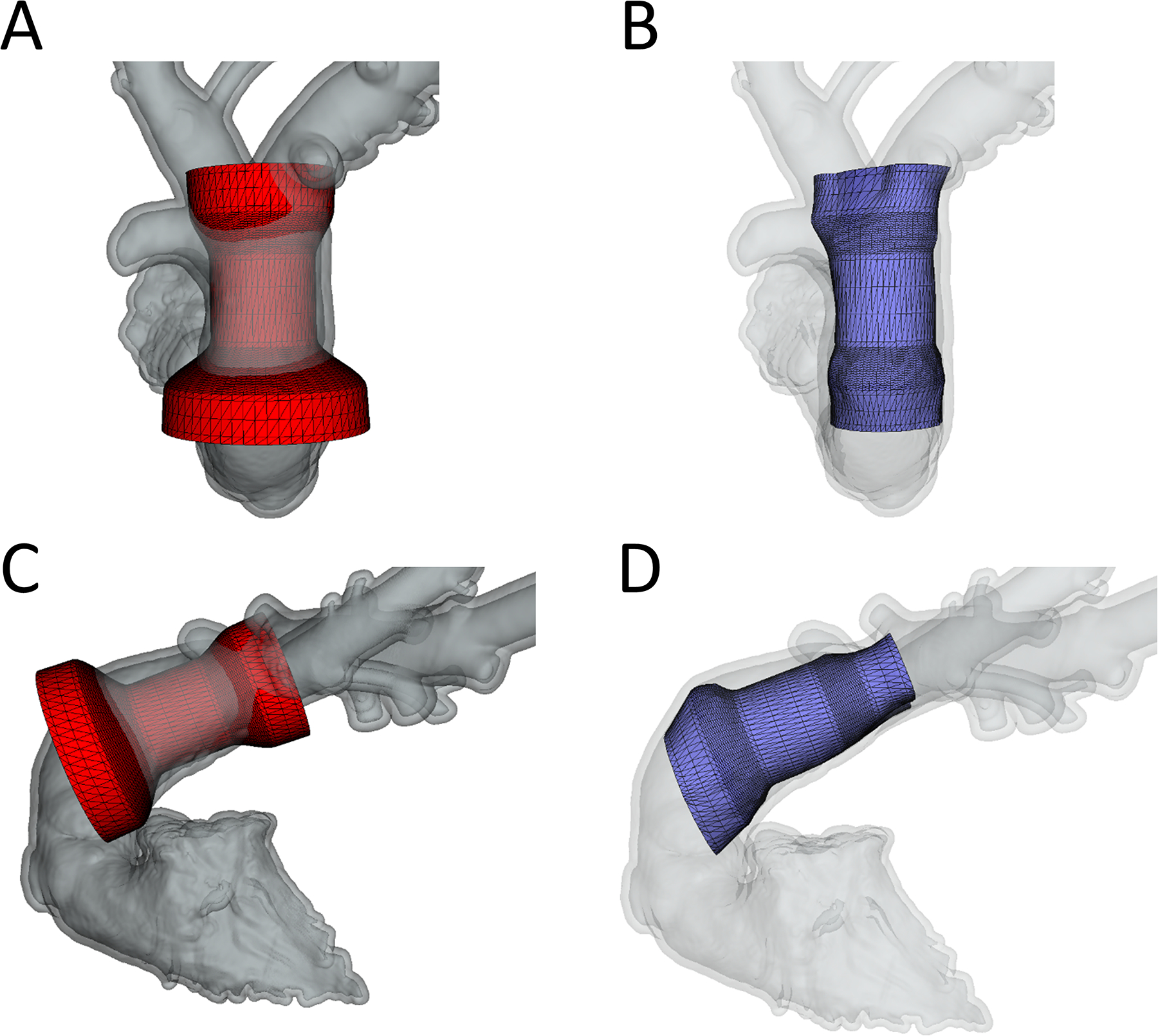
We used custom software to interactively place virtual transcatheter pulmonary valves (TPVs) into RVOT models created from pre-implant and post Harmony valve implant CT scans of 5 ovine surgical models of TOF to quantify and visualize device volume and compression.
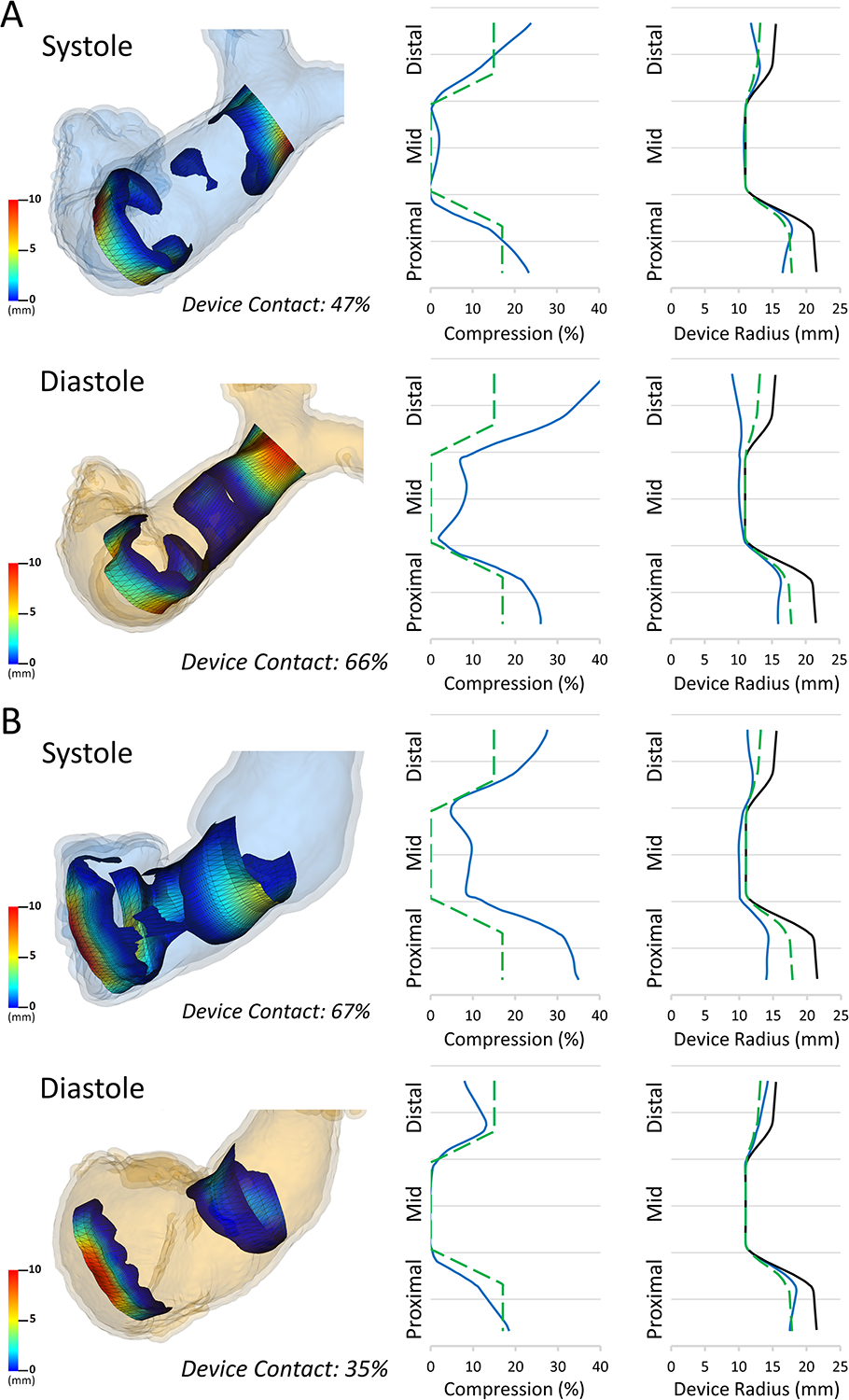
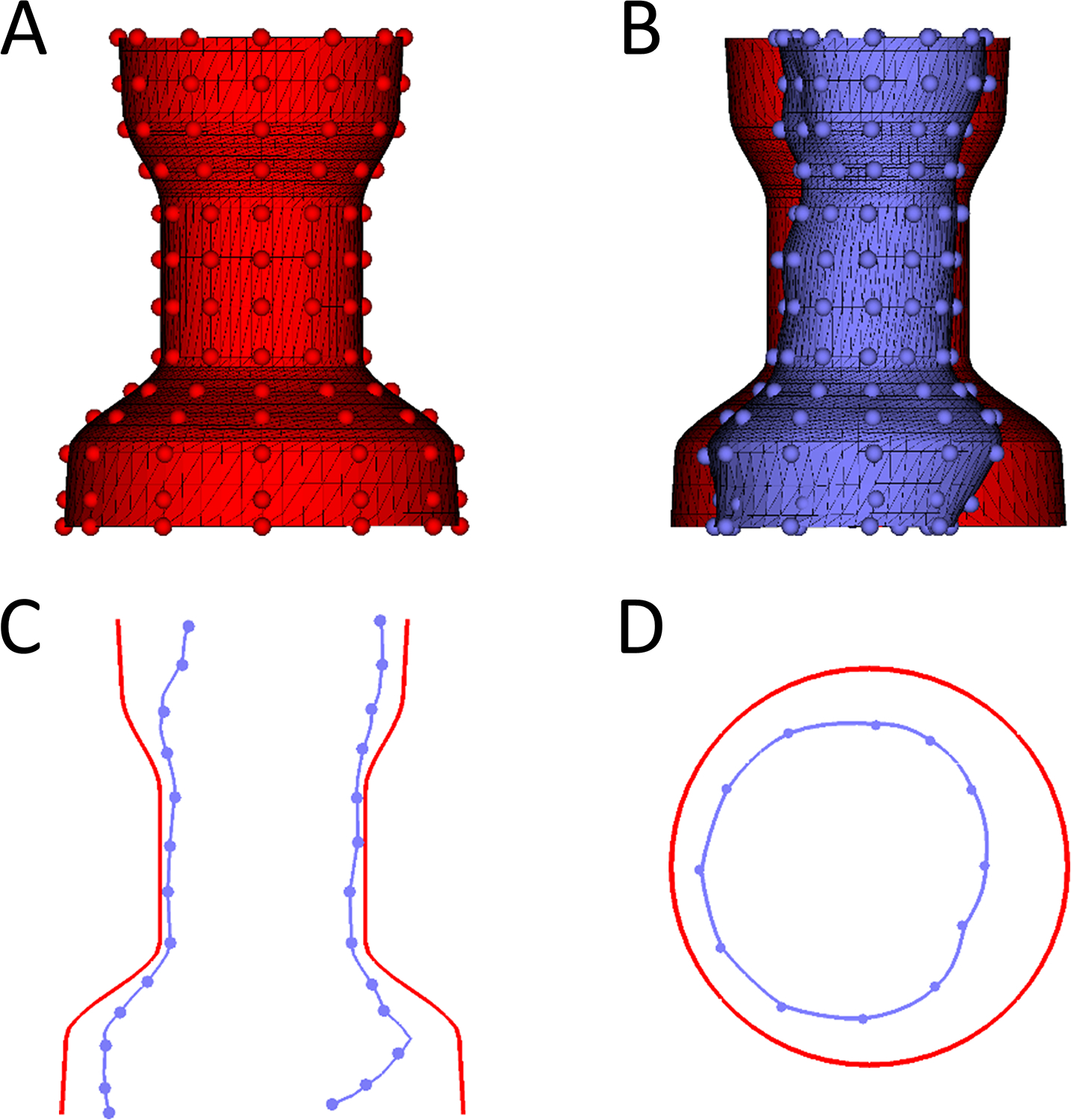
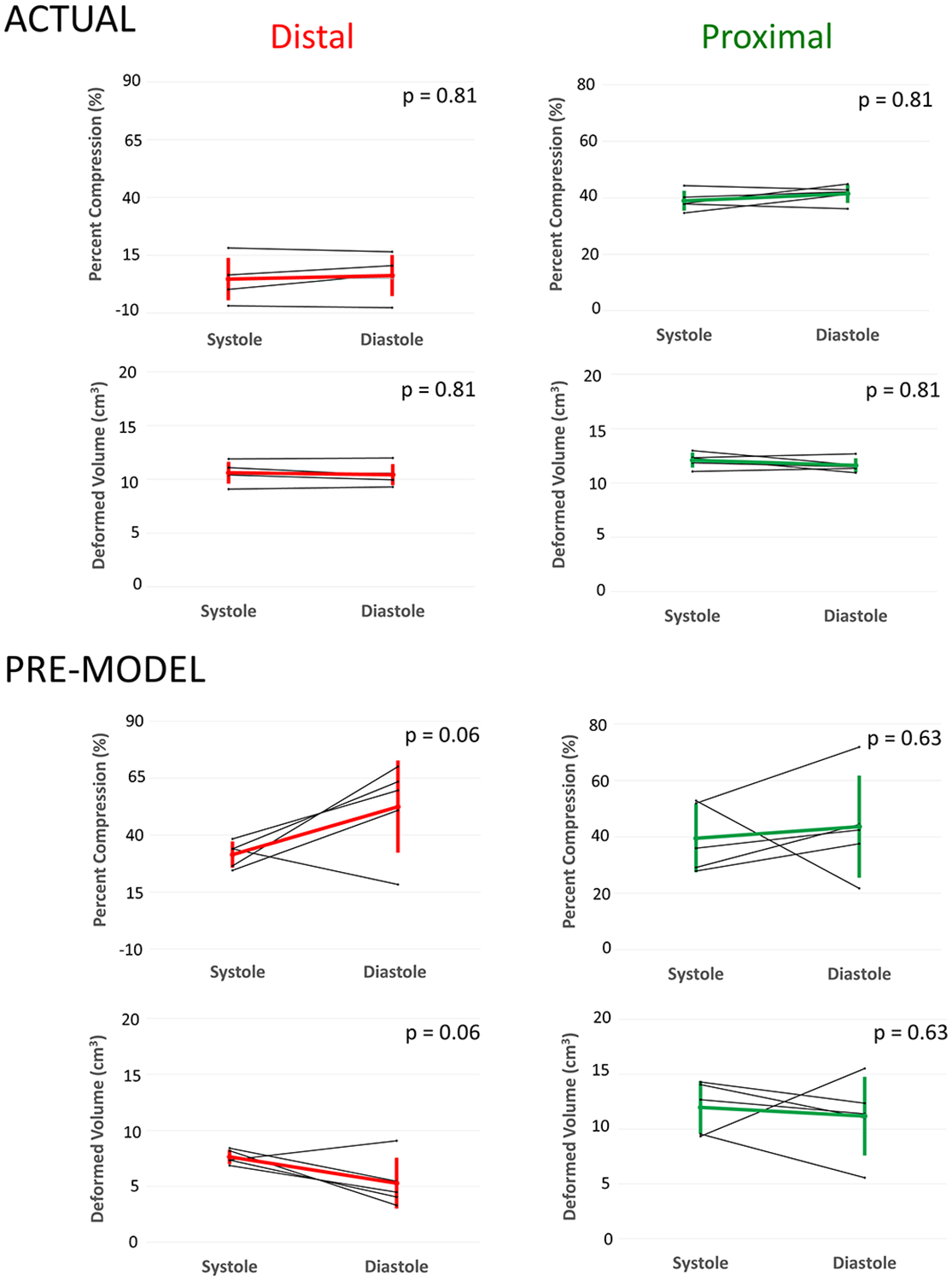
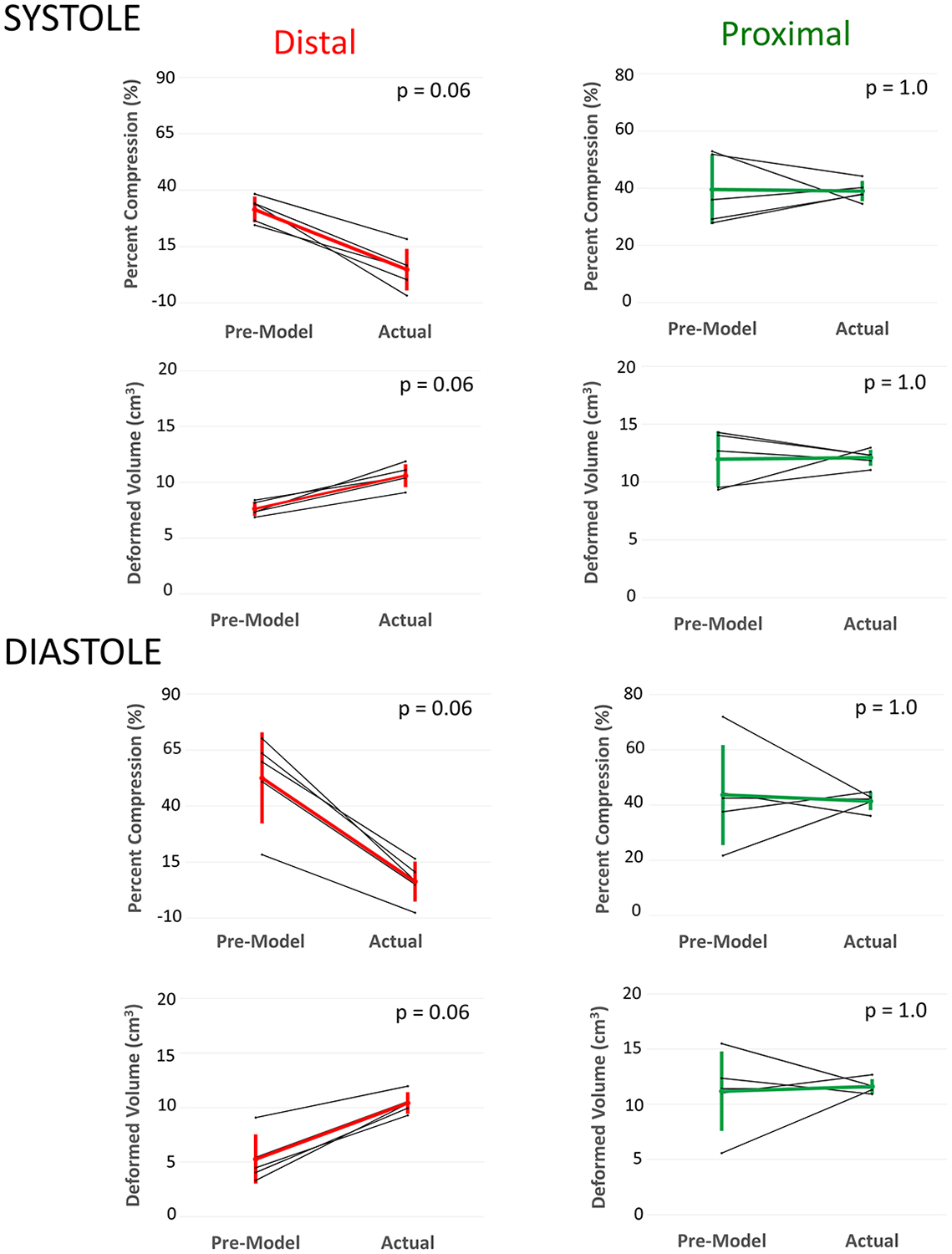
Virtual device placement visually mimicked actual device placement and allowed for quantification of device volume and radius. On average, simulated proximal and distal device volumes and compression did not vary statistically throughout the cardiac cycle (P = 0.11) but assessment was limited by small sample size. In comparison to actual implants, there was no significant pairwise difference in the proximal third of the device (P > 0.80), but the simulated distal device volume was significantly underestimated relative to actual device implant volume (P = 0.06).
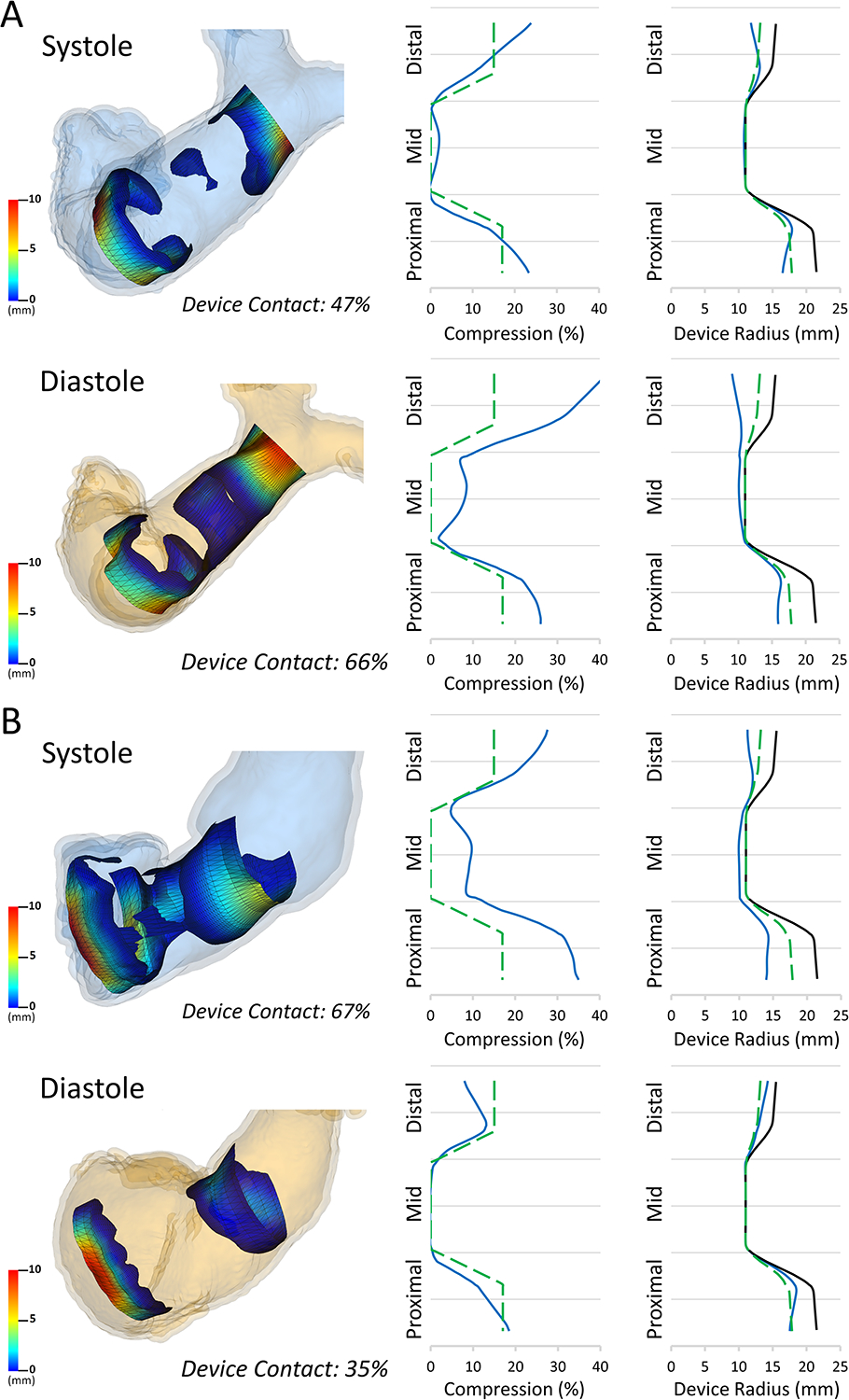
This study demonstrates that pre-implant modeling which assumes a rigid vessel wall may not accurately predict the degree of distal RVOT expansion following actual device placement. We suggest the potential for virtual modeling of TPVR to be a useful adjunct to procedural planning, but further development is needed.
法洛四联症(ToF)经跨环补片修复后可导致肺功能不全,进而导致迟发性发病率和死亡率。经导管原生流出道肺动脉瓣置换术已成为现实。然而,由于右心室流出道(RVOT)的复杂和动态特性,预测一种安全、无创伤的导管设备植入仍然是一个重大挑战。我们试图量化实际植入物和植入前模型预测的压缩和体积差异。
我们使用定制软件将虚拟经导管肺动脉瓣(TPV)交互式地放置在 RVOT 模型中,这些模型是根据 5 只羊手术模型的术前和 Harmony 瓣膜植入后 CT 扫描创建的,用于量化和可视化设备的体积和压缩。
虚拟设备的放置在视觉上模拟了实际设备的放置,并允许对设备体积和半径进行量化。平均而言,模拟近端和远端设备的体积和压缩在整个心动周期中没有统计学差异(P = 0.11),但评估受到样本量小的限制。与实际植入物相比,设备近端三分之一没有显著的两两差异(P > 0.80),但模拟的远端设备体积相对于实际设备植入体积明显低估(P = 0.06)。
本研究表明,假设刚性血管壁的植入前模型可能无法准确预测实际设备放置后 RVOT 远端扩张的程度。我们建议,TPVR 的虚拟建模可能是一种有用的辅助程序规划,但需要进一步发展。