Knecht Talia, Borlongan Cesar, Dela Peña Ike
Department of Pharmaceutical and Administrative Sciences, School of Pharmacy, Loma Linda University, Loma Linda, CA, USA.
Department of Neurosurgery and Brain Repair, Center of Excellence for Aging and Brain Repair, University of South Florida College of Medicine, Tampa, Florida, USA.
Brain Circ. 2018 Jul-Sep;4(3):99-108. doi: 10.4103/bc.bc_21_18. Epub 2018 Oct 9.
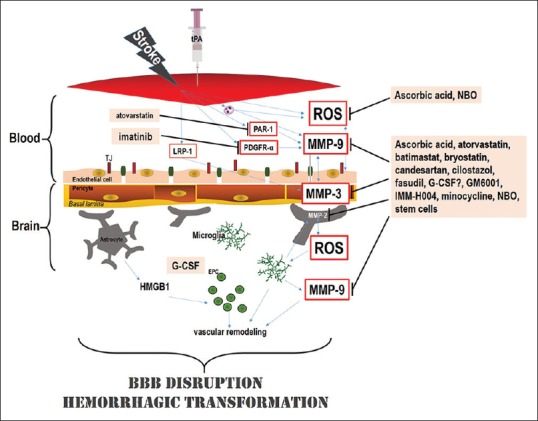
Tissue plasminogen activator (tPA) thrombolysis continues to be the gold standard therapy for ischemic stroke. Due to the time-limited treatment window, within 4.5 h of stroke onset, and a variety of potentially deadly complications related to delayed administration, particularly hemorrhagic transformation (HT), clinical use of tPA is limited. Combination therapies with other interventions, drug or nondrug, have been hypothesized as a logical approach to enhancing tPA effectiveness. Here, we discuss various potential pharmacological and nondrug treatments to minimize adverse effects, primarily HT, associated with delayed tPA administration. Pharmacological interventions include many that support the integrity of the blood-brain barrier (i.e., atorvastatin, batimastat, candesartan, cilostazol, fasudil, and minocycline), promote vascularization and preserve cerebrovasculature (i.e., coumarin derivative IMM-H004 and granulocyte-colony stimulating factor), employing other mechanisms of action (i.e., oxygen transporters and ascorbic acid). Nondrug treatments are comprised of stem cell transplantation and gas therapies with multi-faceted approaches. Combination therapy with tPA and the aforementioned treatments demonstrated promise for mitigating the adverse complications associated with delayed tPA treatment and rescuing stroke-induced behavioral deficits. Therefore, the conjunctive therapy method is a novel therapeutic approach that can attempt to minimize the limitations of tPA treatment and possibly increase the therapeutic window for ischemic stroke treatment.
组织型纤溶酶原激活剂(tPA)溶栓仍然是缺血性中风的金标准治疗方法。由于治疗窗口时间有限,即中风发作后4.5小时内,以及与延迟给药相关的各种潜在致命并发症,特别是出血性转化(HT),tPA的临床应用受到限制。与其他干预措施(药物或非药物)的联合治疗被认为是提高tPA疗效的合理方法。在此,我们讨论各种潜在的药理学和非药物治疗方法,以尽量减少与延迟tPA给药相关的不良反应,主要是HT。药理学干预措施包括许多支持血脑屏障完整性的药物(即阿托伐他汀、batimastat、坎地沙坦、西洛他唑、法舒地尔和米诺环素),促进血管生成并维持脑血管系统的药物(即香豆素衍生物IMM-H004和粒细胞集落刺激因子),以及采用其他作用机制的药物(即氧转运体和抗坏血酸)。非药物治疗包括干细胞移植和气疗法等多方面方法。tPA与上述治疗的联合治疗显示出有望减轻与延迟tPA治疗相关的不良并发症,并挽救中风引起的行为缺陷。因此,联合治疗方法是一种新颖的治疗方法,可尝试尽量减少tPA治疗的局限性,并可能扩大缺血性中风治疗的治疗窗口。