Zeng Wu, Shepard Donald S, Nguyen Ha, Chansa Collins, Das Ashis Kumar, Qamruddin Jumana, Friedman Jed
Schneider Institutes for Health Policy, The Heller School, MS 035, Brandeis University, Waltham, Massachusetts 02454-9110, United States of America (USA).
Health, Nutrition and Population Global Practice, The World Bank Group, Washington DC, USA.
Bull World Health Organ. 2018 Nov 1;96(11):760-771. doi: 10.2471/BLT.17.207100. Epub 2018 Aug 29.
To evaluate the cost-effectiveness of results-based financing and input-based financing to increase use and quality of maternal and child health services in rural areas of Zambia.
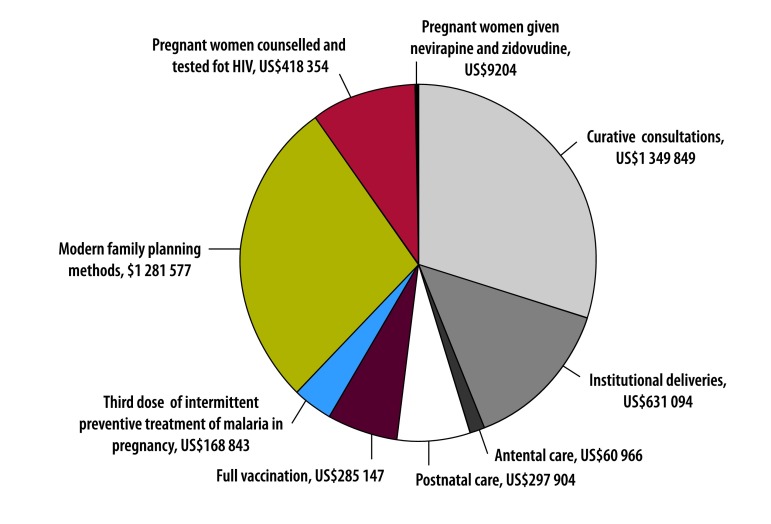
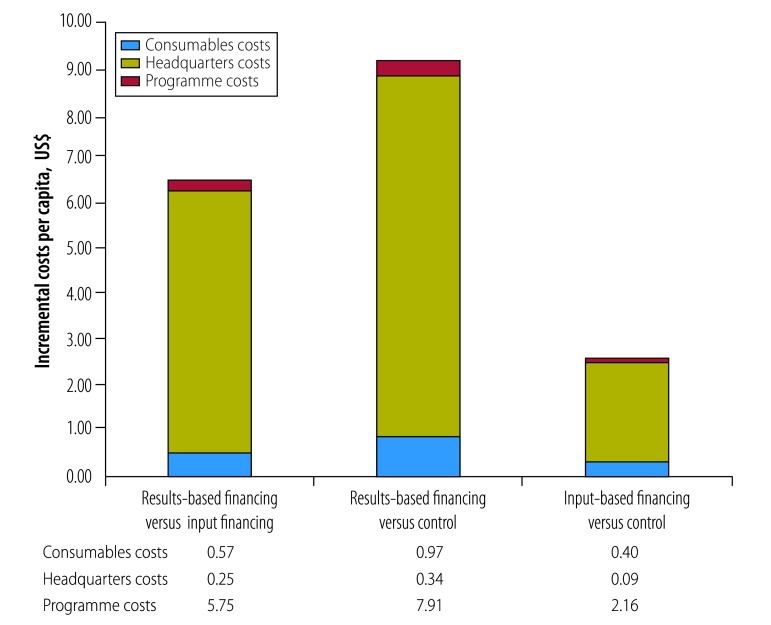
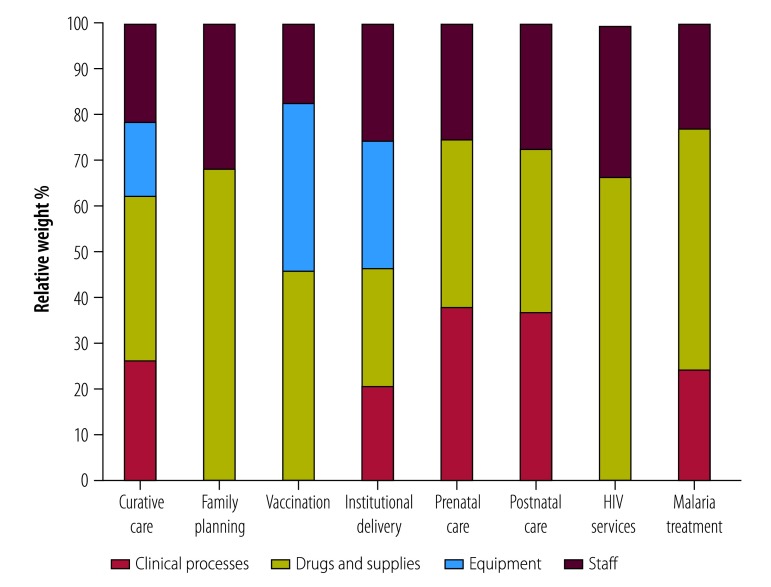
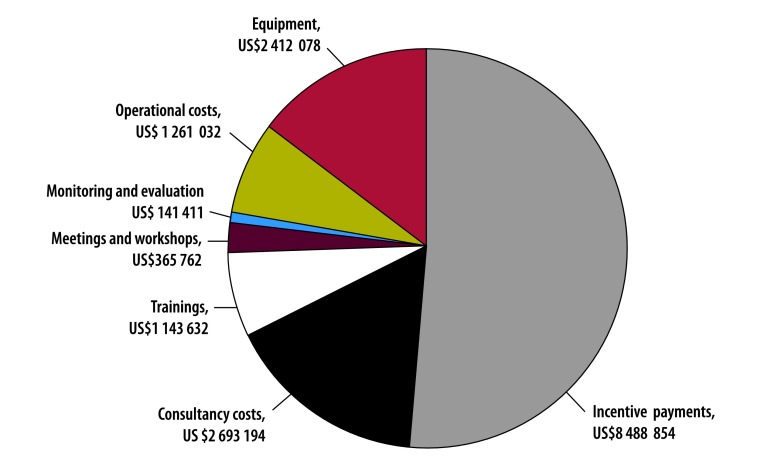
In a cluster-randomized trial from April 2012 to June 2014, 30 districts were allocated to three groups: results-based financing (increased funding tied to performance on pre-agreed indicators), input-based financing (increased funding not tied to performance) or control (no additional funding), serving populations of 1.33, 1.26 and 1.40 million people, respectively. We assessed incremental financial costs for programme implementation and verification, consumables and supervision. We evaluated coverage and quality effectiveness of maternal and child health services before and after the trial, using data from household and facility surveys, and converted these to quality-adjusted life years (QALYs) gained.
Coverage and quality of care increased significantly more in results-based financing than control districts: difference in differences for coverage were 12.8% for institutional deliveries, 8.2% postnatal care, 19.5% injectable contraceptives, 3.0% intermittent preventive treatment in pregnancy and 6.1% to 29.4% vaccinations. In input-based financing districts, coverage increased significantly more versus the control for institutional deliveries (17.5%) and postnatal care (13.2%). Compared with control districts, 641 more lives were saved (lower-upper bounds: 580-700) in results-based financing districts and 362 lives (lower-upper bounds: 293-430) in input-based financing districts. The corresponding incremental cost-effectiveness ratios were 809 United States dollars (US$) and US$ 413 per QALY gained, respectively.
Compared with the control, both results-based financing and input-based financing were cost-effective in Zambia.
评估基于结果的融资和基于投入的融资在提高赞比亚农村地区妇幼保健服务利用率和质量方面的成本效益。
在2012年4月至2014年6月的一项整群随机试验中,30个区被分为三组:基于结果的融资(增加的资金与预先商定指标的绩效挂钩)、基于投入的融资(增加的资金与绩效无关)或对照组(无额外资金),分别服务133万、126万和140万人。我们评估了项目实施、核查、消耗品和监督的增量财务成本。我们利用家庭和机构调查数据评估了试验前后妇幼保健服务的覆盖率和质量效益,并将其转化为获得的质量调整生命年(QALY)。
与对照区相比,基于结果的融资区的护理覆盖率和质量显著提高:机构分娩覆盖率的差异为12.8%,产后护理为8.2%,注射用避孕药为19.5%,孕期间歇性预防治疗为3.0%,疫苗接种为6.1%至29.4%。在基于投入的融资区,机构分娩(17.5%)和产后护理(13.2%)的覆盖率相对于对照组显著提高。与对照区相比,基于结果的融资区多挽救了641条生命(下限-上限:580-700),基于投入的融资区多挽救了362条生命(下限-上限:293-430)。相应的增量成本效益比分别为每获得一个QALY 809美元和413美元。
与对照组相比,基于结果的融资和基于投入的融资在赞比亚均具有成本效益。