Value Evidence and Outcomes, GSK, 980 Great West Road, Brentford, Middlesex, TW8 9GS, UK.
ICON Health Economics, ICON plc, Abingdon, UK.
Respir Res. 2018 Nov 20;19(1):224. doi: 10.1186/s12931-018-0916-7.
A head-to-head study demonstrated the superiority of once-daily umeclidinium bromide/vilanterol (UMEC/VI) 62.5/25 mcg on trough forced expiratory volume in 1 s (FEV) versus once-daily tiotropium/olodaterol (TIO/OLO) 5/5 mcg in symptomatic patients with chronic obstructive pulmonary disease (COPD). This analysis evaluated the cost effectiveness of UMEC/VI versus TIO/OLO from a Spanish National Healthcare System perspective, using data from this study and Spanish literature.
This analysis was conducted from the perspective of the Spanish National Healthcare System with a 3-year horizon as base case. A disease progression model using a linked risk equation approach was used to estimate disease progression and associated healthcare costs, and quality-adjusted life years (QALYs). The Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study was used to develop the statistical risk equations for clinical endpoints, and costs were calculated using a health state approach (by dyspnea severity). Utilities for QALY calculation were estimated using patient baseline characteristics within a regression fit to Spanish observational data. Treatment effect, expressed as change from baseline in FEV was obtained from the head-to-head study and used in the model (UMEC/VI minus TIO/OLO difference: + 52 mL [95% confidence interval: 28, 77]). Baseline patient characteristics were sourced from Spanish literature or the head-to-head study if unavailable. A scenario analysis using only the intent-to-treat (ITT) population from the head-to-head study, and sensitivity analyses (including probabilistic sensitivity analyses), were conducted. Direct healthcare costs (2017 Euro) were obtained from Spanish sources and costs and benefits were discounted at 3% per annum.
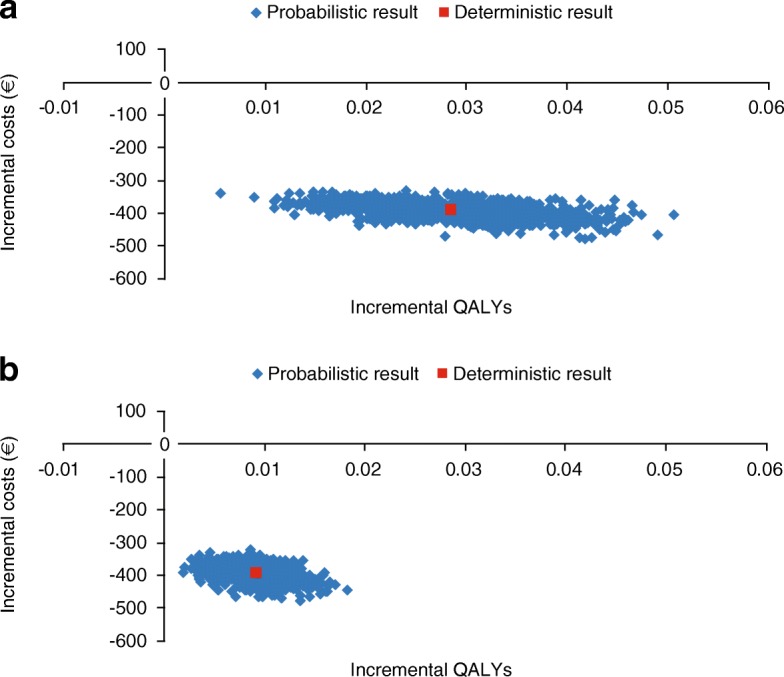
UMEC/VI was associated with small improvements in QALYs (+ 0.029) over a 3-year time horizon, compared with TIO/OLO, alongside cost savings of €393/patient. The ITT scenario analysis and sensitivity analyses had similar results. All probabilistic simulations resulted in UMEC/VI being less costly and more effective than TIO/OLO.
UMEC/VI dominated TIO/OLO (more effective and less expensive). These results may aid payers and decision-makers in Spain when making judgements on which long-acting muscarinic antagonist/long-acting β-agonist (LAMA/LABA) treatments can be considered cost effective in Spain.
一项头对头研究表明,与每日一次噻托溴铵/奥达特罗(TIO/OLO)5/5 mcg 相比,每日一次乌美溴铵/维兰特罗(UMEC/VI)62.5/25 mcg 在慢性阻塞性肺疾病(COPD)症状患者中具有更好的谷值 1 秒用力呼气容积(FEV1)。本分析从西班牙国家医疗保健系统的角度评估了 UMEC/VI 相对于 TIO/OLO 的成本效益,使用了这项研究和西班牙文献中的数据。
本分析以西班牙国家医疗保健系统为视角,以 3 年为基础期。使用链接风险方程方法的疾病进展模型用于估计疾病进展和相关的医疗保健成本,以及调整后的生命年(QALY)。《评估 COPD 纵向以确定预测替代终点(ECLIPSE)》研究用于为临床终点开发统计风险方程,并且使用健康状态方法(按呼吸困难严重程度)计算成本。QALY 计算的效用值使用患者基线特征进行估计,这些特征通过回归拟合到西班牙观察性数据中。使用来自头对头研究的治疗效果,以 FEV 从基线的变化来表示(UMEC/VI 减去 TIO/OLO 的差异:+52 mL[95%置信区间:28,77])。如果无法从西班牙文献或头对头研究中获得患者的基线特征,则从基线特征中获得。使用头对头研究的意向治疗(ITT)人群进行了情景分析,并进行了敏感性分析(包括概率敏感性分析)。直接医疗保健成本(2017 年欧元)来自西班牙来源,成本和效益按每年 3%贴现。
与 TIO/OLO 相比,UMEC/VI 在 3 年时间内与 QALY 略有改善(+0.029),同时患者节省了 393 欧元。ITT 情景分析和敏感性分析得出了类似的结果。所有概率模拟结果均表明,UMEC/VI 的成本低于 TIO/OLO,且效果更好。
UMEC/VI 优于 TIO/OLO(更有效且更经济)。这些结果可能有助于西班牙的支付者和决策者在判断哪些长效抗胆碱能药物/长效β激动剂(LAMA/LABA)治疗在西班牙具有成本效益时做出决策。