School of Health and Biomedical Sciences, RMIT University, Melbourne, VIC, Australia.
Front Immunol. 2018 Oct 16;9:2345. doi: 10.3389/fimmu.2018.02345. eCollection 2018.
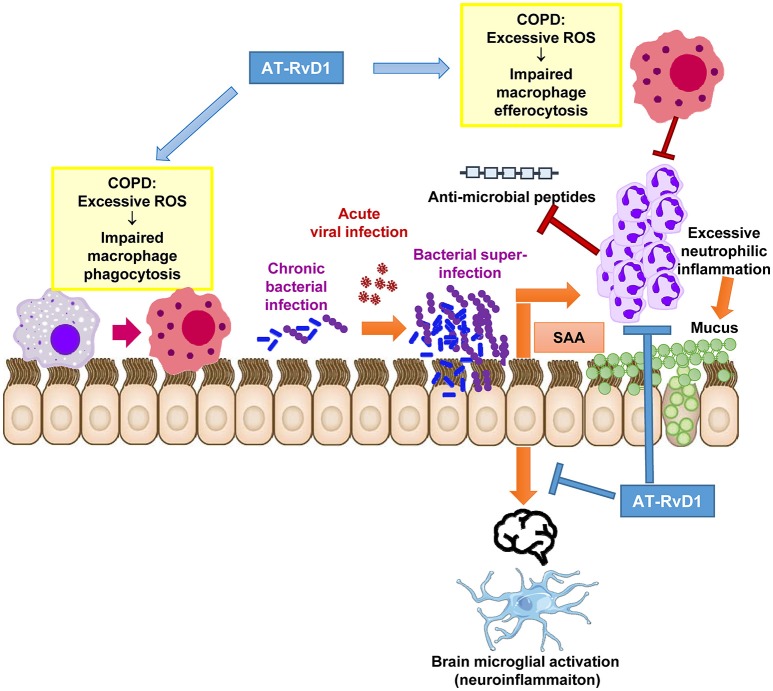
Chronic obstructive pulmonary disease (COPD) is a leading cause of disability and death world-wide, where chronic inflammation accelerates lung function decline. Pathological inflammation is worsened by chronic bacterial lung infections and susceptibility to recurrent acute exacerbations of COPD (AECOPD), typically caused by viral and/or bacterial respiratory pathogens. Despite ongoing efforts to reduce AECOPD rates with inhaled corticosteroids, COPD patients remain at heightened risk of developing serious lung infections/AECOPD, frequently leading to hospitalization and infection-dependent delirium. Here, we review emerging mechanisms into why COPD patients are susceptible to chronic bacterial infections and highlight dysregulated inflammation and production of reactive oxygen species (ROS) as central causes. This underlying chronic infection leaves COPD patients particularly vulnerable to acute viral infections, which further destabilize host immunity to bacteria. The pathogeneses of bacterial and viral exacerbations are significant as clinical symptoms are more severe and there is a marked increase in neutrophilic inflammation and tissue damage. AECOPD triggered by a bacterial and viral co-infection increases circulating levels of the systemic inflammatory marker, serum amyloid A (SAA). SAA is a functional agonist for formyl peptide receptor 2 (FPR2/ALX), where it promotes chemotaxis and survival of neutrophils. Excessive levels of SAA can antagonize the protective actions of FPR2/ALX that involve engagement of specialized pro-resolving mediators, such as resolvin-D1. We propose that the anti-microbial and anti-inflammatory actions of specialized pro-resolving mediators, such as resolvin-D1 should be harnessed for the treatment of AECOPD that are complicated by the co-pathogenesis of viruses and bacteria.
慢性阻塞性肺疾病(COPD)是全球范围内导致残疾和死亡的主要原因,其中慢性炎症加速了肺功能下降。慢性细菌肺部感染和易发生 COPD 急性加重(AECOPD)会使病理性炎症恶化,AECOPD 通常由病毒和/或细菌呼吸道病原体引起。尽管人们一直在努力通过吸入皮质类固醇降低 AECOPD 发生率,但 COPD 患者仍面临发生严重肺部感染/AECOPD 的高风险,这经常导致住院和感染相关的意识混乱。在这里,我们综述了 COPD 患者易发生慢性细菌感染的新机制,并强调了失调的炎症和活性氧(ROS)产生是主要原因。这种潜在的慢性感染使 COPD 患者特别容易受到急性病毒感染的影响,进一步破坏了宿主对细菌的免疫。细菌和病毒加重的发病机制非常重要,因为临床症状更严重,中性粒细胞炎症和组织损伤明显增加。细菌和病毒的混合感染引起的 AECOPD 会增加循环系统中炎症标志物血清淀粉样蛋白 A(SAA)的水平。SAA 是甲酰肽受体 2(FPR2/ALX)的功能性激动剂,它促进中性粒细胞的趋化和存活。SAA 水平过高会拮抗 FPR2/ALX 的保护作用,涉及特殊的促解决介质,如 resolvin-D1 的参与。我们提出,专门的促解决介质,如 resolvin-D1 的抗微生物和抗炎作用,应该被利用来治疗由病毒和细菌共同引起的 AECOPD。