Fricke K, Schneider H, Biselli P, Hansel N N, Zhang Z G, Sowho M O, Grote L
Department of Medicine, Division of Pulmonary and Critical Care Medicine, Johns Hopkins School of Medicine, Baltimore, MD, USA,
Department for Pulmonary, Sleep, and Intensive Care Medicine, Helios Klinikum, Wuppertal, Germany.
Int J Chron Obstruct Pulmon Dis. 2018 Nov 2;13:3635-3643. doi: 10.2147/COPD.S166093. eCollection 2018.
Patients with COPD have increased respiratory loads and altered blood gases, both of which affect vascular function and sympathetic activity. Sleep, particularly rapid eye movement (REM) sleep, is known to exacerbate hypoxia and respiratory loads. Therefore, we hypothesize that nasal high flow (NHF), which lowers ventilatory loads, reduces sympathetic activity during sleep and that this effect depends on COPD severity.
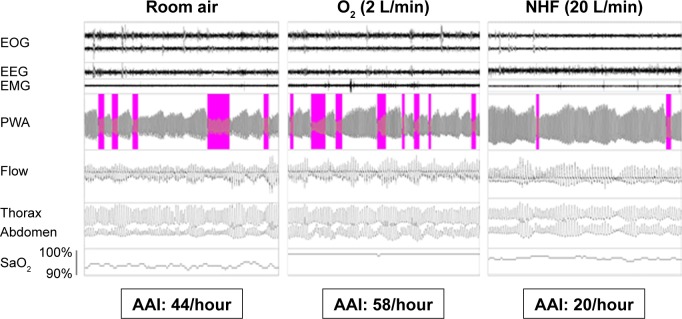
We performed full polysomnography in COPD patients (n=17; FEV, 1.6±0.6 L) and in matched controls (n=8). Participants received room air (RA) at baseline and single night treatment with O (2 L/min) and NHF (20 L/min) in a random order. Finger pulse wave amplitude (PWA), a measure of vascular sympathetic tone, was assessed by photoplethysmography. Autonomic activation (AA) events were defined as PWA attenuation ≥30% and indexed per hour for sleep stages (AA index [AAI]) at RA, NHF, and O).
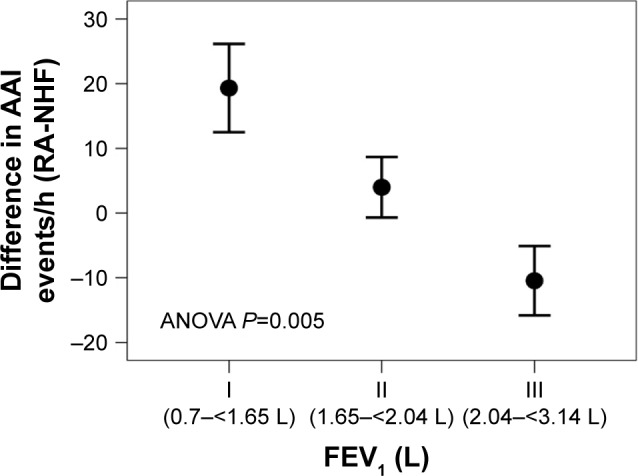
In COPD, sleep apnea improved following O (REM-apnea hypopnea index [AHI] with RA, O, and NHF: 18.6±20.9, 12.7±18.1, and 14.4±19.8, respectively; =0.04 for O and =0.06 for NHF). REM-AAI was reduced only following NHF in COPD patients (AAI-RA, 21.5±18.4 n/h and AAI-NHF, 9.9±6.8 n/h, =0.02) without changes following O (NHF-O difference, =0.01). REM-AAI reduction was associated with lung function expressed as FEV and FVC (FEV: =-0.59, =0.001; FEV/FVC: =-0.52 and =0.007).
NHF but not elevated oxygenation reduces peripheral vascular sympathetic activity in COPD patients during REM sleep. Sympathetic off-loading by NHF, possibly related to improved breathing mechanics, showed a strong association with COPD severity.
慢性阻塞性肺疾病(COPD)患者的呼吸负荷增加且血气改变,这两者均会影响血管功能和交感神经活动。已知睡眠,尤其是快速眼动(REM)睡眠,会加重缺氧和呼吸负荷。因此,我们推测,降低通气负荷的经鼻高流量(NHF)会降低睡眠期间的交感神经活动,且这种作用取决于COPD的严重程度。
我们对COPD患者(n = 17;第1秒用力呼气容积[FEV₁]为1.6±0.6 L)和匹配的对照组(n = 8)进行了全夜多导睡眠监测。参与者在基线时接受室内空气(RA),并随机接受单夜O₂(2 L/min)和NHF(20 L/min)治疗。通过光电容积描记法评估作为血管交感神经张力指标的手指脉搏波振幅(PWA)。自主神经激活(AA)事件定义为PWA衰减≥30%,并按每小时睡眠阶段进行索引(RA、NHF和O₂时的AA指数[AAI])。
在COPD患者中,O₂治疗后睡眠呼吸暂停有所改善(RA、O₂和NHF时的REM-呼吸暂停低通气指数[AHI]分别为18.6±20.9、12.7±18.1和14.4±19.8;O₂时P = 0.04,NHF时P = 0.06)。COPD患者仅在接受NHF治疗后REM-AAI降低(AAI-RA为21.5±18.4次/小时,AAI-NHF为9.9±6.8次/小时,P = 0.02),而接受O₂治疗后无变化(NHF与O₂的差异,P = 0.01)。REM-AAI降低与以FEV₁和用力肺活量(FVC)表示的肺功能相关(FEV₁:P = -0.59,P = 0.001;FEV₁/FVC:P = -0.52,P = 0.007)。
在COPD患者的REM睡眠期间,NHF可降低外周血管交感神经活动,而提高氧合则不能。NHF减轻交感神经负荷,可能与呼吸力学改善有关,且与COPD严重程度密切相关。