Otsuka Taiga, Kawaguchi Yasunori, Mizuta Toshihiko, Ide Yasushi, Koga Futa, Kumagai Takanori, Yoshioka Wataru, Murayama Kenichiro, Rikitake Osamu, Ikeda Yuji, Ozaki Iwata
Department of Internal Medicine, Division of Hepatology Saga University Hospital Saga Japan.
Hepato-Biliary and Pancreatology Division Saga Medical Center Koseikan Saga Japan.
JGH Open. 2017 Nov 28;1(4):148-152. doi: 10.1002/jgh3.12026. eCollection 2017 Dec.
Patients requiring hemodialysis show high morbidity with hepatitis C virus (HCV) infection, but there are difficulties associated with interferon-based therapies. Asunaprevir and daclatasvir could help patients with HCV genotype 1b because the drugs have a nonrenal metabolism and show good viral eradication. We evaluated the efficacy and safety of combined asunaprevir and daclatasvir therapy.
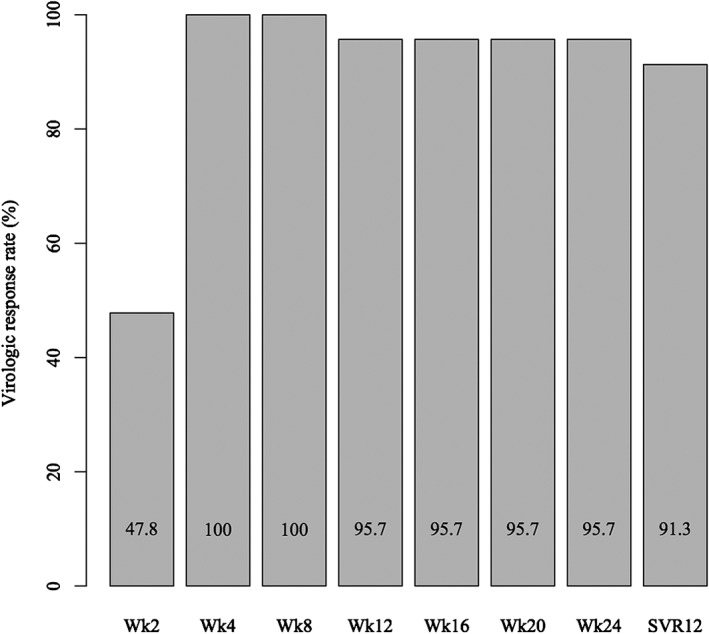
This was a multicenter prospective trial of patients with chronic hepatitis or compensated cirrhosis from HCV genotype 1b who had end-stage renal disease requiring chronic hemodialysis. Asunaprevir and daclatasvir were administered orally (100 mg twice daily and 60 mg once daily, respectively) for 24 weeks. The primary end-point was the proportion of patients achieving sustained virological response 12, defined as HCV RNA <15 IU/mL undetectable at 12 weeks after completion of asunaprevir and daclatasvir treatment.
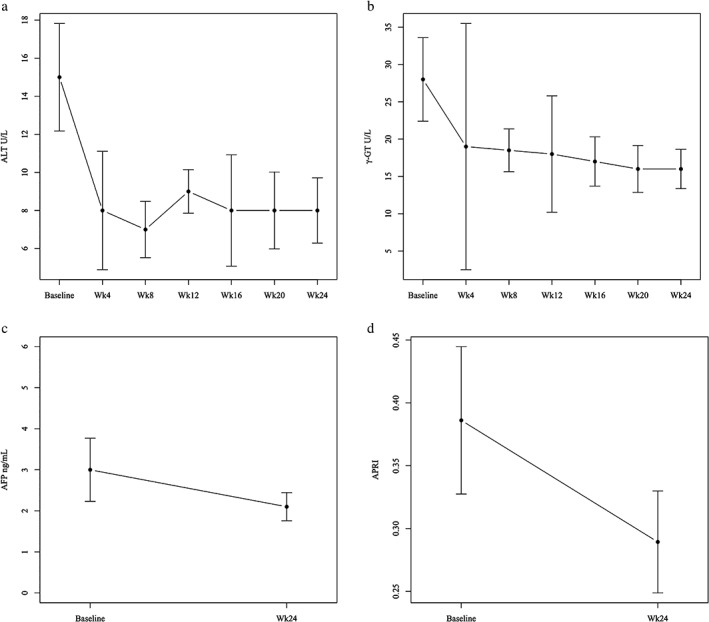
Between December 2014 and December 2015, 23 dialysis patients were enrolled, and 22 patients completed the protocol therapy. Sustained virological response 12 rates were 91.3% (95% confidence interval: 72.0-98.9) in the intention-to-treat and 95.5% (95% confidence interval: 77.2-99.9) in the per-protocol populations. Serum aminotransferase significantly decreased after initiation of asunaprevir and daclatasvir ( < 0.01), although the level was low at baseline. Asunaprevir and daclatasvir were well tolerated; however, one patient could not continue because of infective endocarditis and cerebral infarction.
Asunaprevir and daclatasvir could help patients with chronic hepatitis C receiving hemodialysis. Close collaboration with dialysis physicians is important when treating these patients because hemodialysis carries life-threatening risks.
需要进行血液透析的患者丙型肝炎病毒(HCV)感染发病率很高,但基于干扰素的治疗存在困难。asunaprevir和daclatasvir对丙型肝炎病毒1b型患者可能有效,因为这两种药物通过非肾脏途径代谢,且显示出良好的病毒清除效果。我们评估了asunaprevir与daclatasvir联合治疗的疗效和安全性。
这是一项针对丙型肝炎病毒1b型慢性肝炎或代偿期肝硬化且患有需要长期血液透析的终末期肾病患者的多中心前瞻性试验。口服asunaprevir和daclatasvir(分别为每日两次,每次100毫克和每日一次,每次60毫克),持续24周。主要终点是实现持续病毒学应答12的患者比例,定义为在asunaprevir和daclatasvir治疗完成后12周时检测不到HCV RNA<15 IU/mL。
在2014年12月至2015年12月期间,23名透析患者入组,22名患者完成了方案治疗。在意向性分析人群中,持续病毒学应答12率为91.3%(95%置信区间:72.0 - 98.9),符合方案人群中为95.5%(95%置信区间:77.2 - 99.9)。在开始使用asunaprevir和daclatasvir后,血清转氨酶显著下降(<0.01),尽管基线时水平较低。asunaprevir和daclatasvir耐受性良好;然而,有一名患者因感染性心内膜炎和脑梗死无法继续治疗。
asunaprevir和daclatasvir可能有助于接受血液透析的慢性丙型肝炎患者。在治疗这些患者时,与透析医生密切合作很重要,因为血液透析存在危及生命的风险。