Dirnena-Fusini Ilze, Åm Marte Kierulf, Fougner Anders Lyngvi, Carlsen Sven Magnus, Christiansen Sverre Christian
Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Sciences, NTNU - Norwegian University of Science and Technology, Trondheim, Norway.
Department of Endocrinology, St Olavs Hospital, Trondheim, Norway.
BMJ Open Diabetes Res Care. 2018 Nov 9;6(1):e000560. doi: 10.1136/bmjdrc-2018-000560. eCollection 2018.
Hypoglycemia is a frequent and potentially dangerous event among patients with diabetes mellitus type 1. Subcutaneous glucagon is an emergency treatment to counteract severe hypoglycemia. The effect of intraperitoneal glucagon delivery is sparsely studied. We performed a direct comparison of the blood glucose response following intraperitoneally, subcutaneously and intravenously administered glucagon.
This is a prospective, randomized, controlled, open-label, crossover trial in 20 octreotide-treated rats. Three interventions, 1 week apart, in a randomized order, were done in each rat. All 20 rats were given intraperitoneal and subcutaneous glucagon injections, from which 5 rats were given intravenous glucagon injections and 15 rats received placebo (intraperitoneal isotonic saline) injection. The dose of glucagon was 5 µg/kg body weight for all routes of administration. Blood glucose levels were measured before and until 60 min after the glucagon/placebo injections.
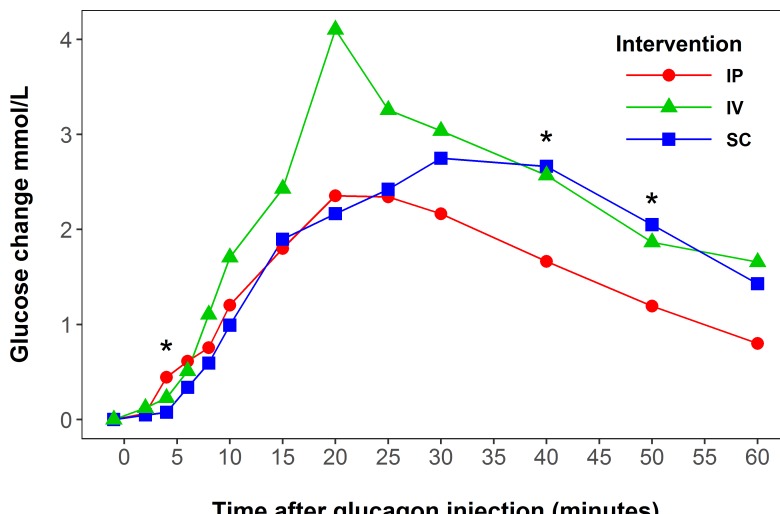
Compared with placebo-treated rats, a significant increase in blood glucose was observed 4 min after intraperitoneal glucagon administration (p=0.009), whereas after subcutaneous and intravenous glucagon administration significant increases were seen after 8 min (p=0.002 and p<0.001, respectively). In intraperitoneally treated compared with subcutaneously treated rats, the increase in blood glucose was higher after 4 min (p=0.019) and lower after 40 min (p=0.005) and 50 min (p=0.011). The maximum glucose response occurred earlier after intraperitoneal compared with subcutaneous glucagon injection (25 min vs 35 min; p=0.003).
Glucagon administered intraperitoneally gives a faster glucose response compared with subcutaneously administered glucagon in rats. If repeatable in humans, the more rapid glucose response may be of importance in a dual-hormone artificial pancreas using the intraperitoneal route for administration of insulin and glucagon.
低血糖是1型糖尿病患者中常见且可能危险的事件。皮下注射胰高血糖素是对抗严重低血糖的一种紧急治疗方法。腹腔内注射胰高血糖素的效果研究较少。我们对腹腔内、皮下和静脉注射胰高血糖素后的血糖反应进行了直接比较。
这是一项针对20只接受奥曲肽治疗的大鼠的前瞻性、随机、对照、开放标签、交叉试验。每只大鼠按随机顺序进行三种干预,每次干预间隔1周。所有20只大鼠均接受腹腔内和皮下注射胰高血糖素,其中5只大鼠接受静脉注射胰高血糖素,15只大鼠接受安慰剂(腹腔内注射等渗盐水)注射。所有给药途径的胰高血糖素剂量均为5μg/kg体重。在注射胰高血糖素/安慰剂之前及之后直至60分钟测量血糖水平。
与接受安慰剂治疗的大鼠相比,腹腔内注射胰高血糖素后4分钟血糖显著升高(p=0.009),而皮下和静脉注射胰高血糖素后8分钟血糖显著升高(分别为p=0.002和p<0.001)。与皮下注射治疗的大鼠相比,腹腔内治疗的大鼠在4分钟后血糖升高更高(p=0.019),在40分钟(p=0.005)和50分钟(p=0.011)后血糖升高更低。与皮下注射胰高血糖素相比,腹腔内注射胰高血糖素后最大血糖反应出现得更早(25分钟对35分钟;p=0.003)。
与皮下注射胰高血糖素相比,大鼠腹腔内注射胰高血糖素能使血糖反应更快。如果在人类中也具有可重复性,那么在使用腹腔途径给药胰岛素和胰高血糖素的双激素人工胰腺中,更快的血糖反应可能具有重要意义。