1 Durham VA Health Care System, Durham, NC, USA.
2 Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine, Durham, NC, USA.
Palliat Med. 2019 Feb;33(2):123-134. doi: 10.1177/0269216318812633. Epub 2018 Nov 29.
: Despite increasing emphasis on integration of palliative care with disease-directed care for advanced cancer, the nature of this integration and its effects on patient and caregiver outcomes are not well-understood.
: We evaluated the effects of integrated outpatient palliative and oncology care for advanced cancer on patient and caregiver outcomes.
: Following a standard protocol (PROSPERO: CRD42017057541), investigators independently screened reports to identify randomized controlled trials or quasi-experimental studies that evaluated the effect of integrated outpatient palliative and oncology care interventions on quality of life, survival, and healthcare utilization among adults with advanced cancer. Data were synthesized using random-effects meta-analyses, supplemented with qualitative methods when necessary.
: English-language peer-reviewed publications in PubMed, CINAHL, and Cochrane Central through November 2016. We subsequently updated our PubMed search through July 2018.
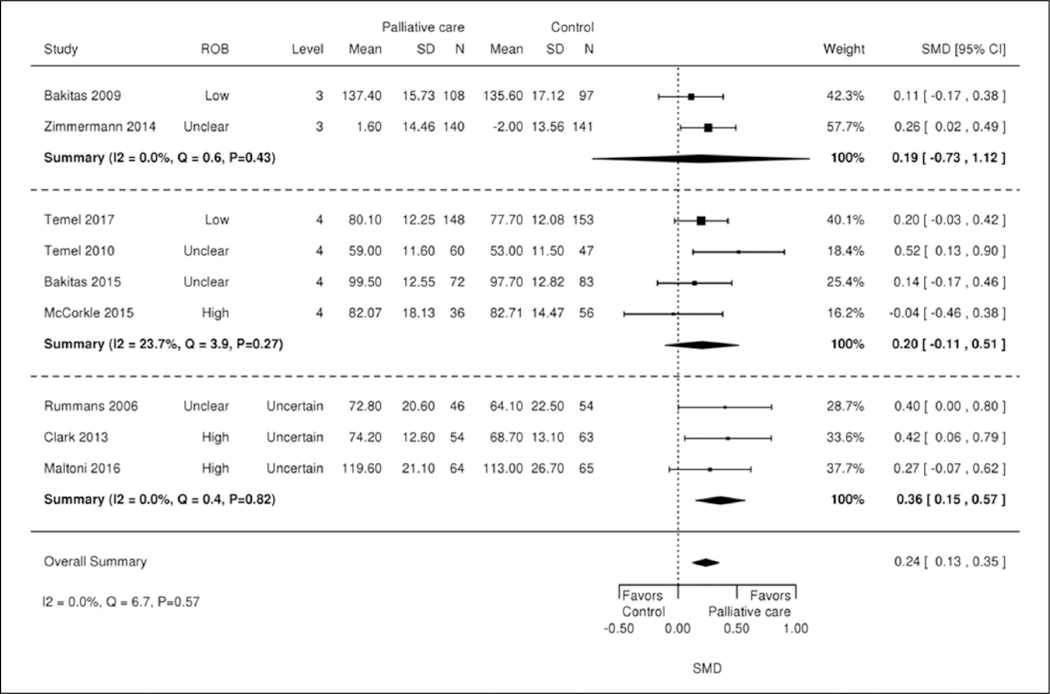
: Eight randomized-controlled and two cluster-randomized trials were included. Most patients had multiple advanced cancers, with median time from diagnosis or recurrence to enrollment ranging from 8 to 12 weeks. All interventions included a multidisciplinary team, were classified as “moderately integrated,” and addressed physical and psychological symptoms. In a meta-analysis, short-term quality of life improved, symptom burden improved, and all-cause mortality decreased. Qualitative analyses revealed no association between integration elements, palliative care intervention elements, and intervention impact. Utilization and caregiver outcomes were often not reported.
: Moderately integrated palliative and oncology outpatient interventions had positive effects on short-term quality of life, symptom burden, and survival. Evidence for effects on healthcare utilization and caregiver outcomes remains sparse.
尽管越来越重视将姑息治疗与晚期癌症的疾病导向治疗相结合,但这种整合的性质及其对患者和护理人员结局的影响仍未得到很好的理解。
我们评估了针对晚期癌症的姑息治疗与肿瘤学整合门诊治疗对患者和护理人员结局的影响。
按照标准方案(PROSPERO:CRD42017057541),研究人员独立筛选报告,以确定评估姑息治疗与肿瘤学整合门诊干预对晚期癌症成人生活质量、生存和医疗保健利用影响的随机对照试验或准实验研究。使用随机效应荟萃分析综合数据,在必要时辅以定性方法。
PubMed、CINAHL 和 Cochrane Central 的英文同行评审出版物,检索时间截至 2016 年 11 月。随后,我们通过 2018 年 7 月更新了 PubMed 检索。
纳入 8 项随机对照试验和 2 项整群随机试验。大多数患者患有多种晚期癌症,从诊断或复发到入组的中位时间为 8 至 12 周。所有干预措施均包括多学科团队,被归类为“中度整合”,并解决了身体和心理症状。荟萃分析显示,短期生活质量改善,症状负担减轻,全因死亡率降低。定性分析显示,整合要素、姑息治疗干预要素与干预效果之间无关联。利用率和护理人员结局通常未报告。
姑息治疗与肿瘤学整合门诊干预对短期生活质量、症状负担和生存有积极影响。关于对医疗保健利用率和护理人员结局影响的证据仍然稀少。