Tana Milena, Lio Alessandra, Tirone Chiara, Aurilia Claudia, Tiberi Eloisa, Serrao Francesca, Purcaro Velia, Corsello Mirta, Catenazzi Piero, D'Andrea Vito, Barone Giovanni, Ricci Cinzia, Pastorino Roberta, Vento Giovanni
Unità Operativa Complessa di Neonatologia, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy.
Section of Hygiene, Institute of Public Health, Università Cattolica del Sacro Cuore, Rome, Italy.
BMJ Paediatr Open. 2018 Nov 9;2(1):e000350. doi: 10.1136/bmjpo-2018-000350. eCollection 2018.
To evaluate if weaning from high-frequency oscillatory ventilation (HFOV) directly to a non-invasive mode of respiratory support is feasible and results in successful extubation in extremely low birth weight (ELBW) infants.
Prospective observational study.
Tertiary neonatal intensive care unit.
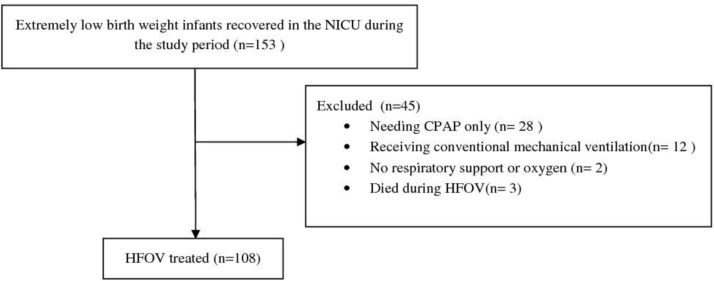
One hundred and eight ELBW infants of 26.2±1.4 weeks of gestational age (GA) directly extubated from HFOV.
All infants were managed with elective HFOV and received surfactant after a recruitment HFOV manoeuvre. Extubation was attempted at mean airways pressure (MAP) ≤6 cm HO with FiO ≤0.25. After extubation, all infants were supported by nasal continuous positive airway pressure (6-8 cm HO).
Extubation failure (clinical deterioration requiring reintubation) was defined as shorter than 7 days.
Ninety patients (83%) were successfully extubated and 18 (17%) required reintubation. No significant differences were found between the two groups in terms of birth weight, day of life and weight at the time of extubation. Multivariable analysis showed that GA (OR 1.71; 95% CI 1.04, 2.08) and higher MAP prior to surfactant (OR 1.51; 95% CI 1.06, 2.15) were associated with successful extubation.
In ELBW infants, direct extubation from HFOV at MAP ≤6 cm HO with FiO ≤0.25 is feasible. Our extubation success rate (83%) is higher than conventional mechanical ventilation in this very vulnerable class of infants.
评估极低出生体重(ELBW)婴儿从高频振荡通气(HFOV)直接撤机至无创呼吸支持模式是否可行,以及能否成功拔管。
前瞻性观察性研究。
三级新生儿重症监护病房。
108例胎龄26.2±1.4周的ELBW婴儿,直接从HFOV撤机。
所有婴儿均接受选择性HFOV治疗,并在进行复张HFOV操作后给予表面活性剂。在平均气道压(MAP)≤6 cm HO且吸入氧分数(FiO)≤0.25时尝试拔管。拔管后,所有婴儿均接受经鼻持续气道正压通气(6 - 8 cm HO)支持。
拔管失败(临床病情恶化需要重新插管)定义为时间短于7天。
90例患者(83%)成功拔管,18例(17%)需要重新插管。两组在出生体重、日龄和拔管时体重方面无显著差异。多变量分析显示,胎龄(比值比[OR] 1.71;95%置信区间[CI] 1.04,2.08)和使用表面活性剂前较高的MAP(OR 1.51;95% CI 1.06,2.15)与成功拔管相关。
对于ELBW婴儿,在MAP≤6 cm HO且FiO≤0.25时从HFOV直接拔管是可行的。在这类极易患病的婴儿中,我们的拔管成功率(83%)高于传统机械通气。