Department of Computer Sciences and Engineering, University of South Florida, Tampa, Florida.
Department of Cancer Physiology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, Florida.
Cancer Med. 2018 Dec;7(12):6340-6356. doi: 10.1002/cam4.1852. Epub 2018 Dec 1.
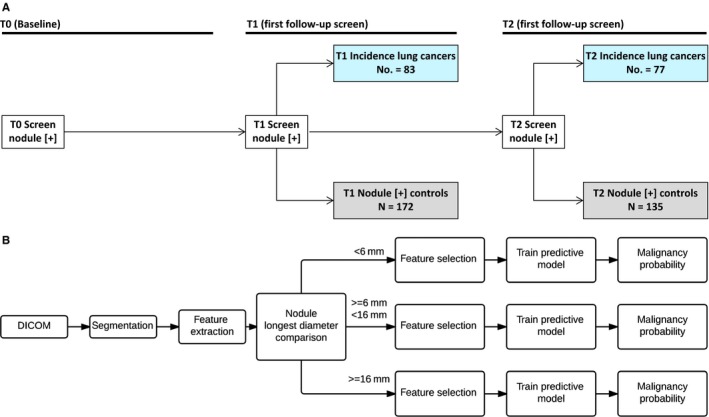
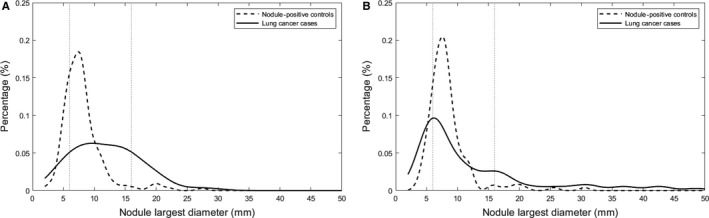
Current guidelines for lung cancer screening increased a positive scan threshold to a 6 mm longest diameter. We extracted radiomic features from baseline and follow-up screens and performed size-specific analyses to predict lung cancer incidence using three nodule size classes (<6 mm [small], 6-16 mm [intermediate], and ≥16 mm [large]).
We extracted 219 features from baseline (T0) nodules and 219 delta features which are the change from T0 to first follow-up (T1). Nodules were identified for 160 incidence cases diagnosed with lung cancer at T1 or second follow-up screen (T2) and for 307 nodule-positive controls that had three consecutive positive screens not diagnosed as lung cancer. The cases and controls were split into training and test cohorts; classifier models were used to identify the most predictive features.
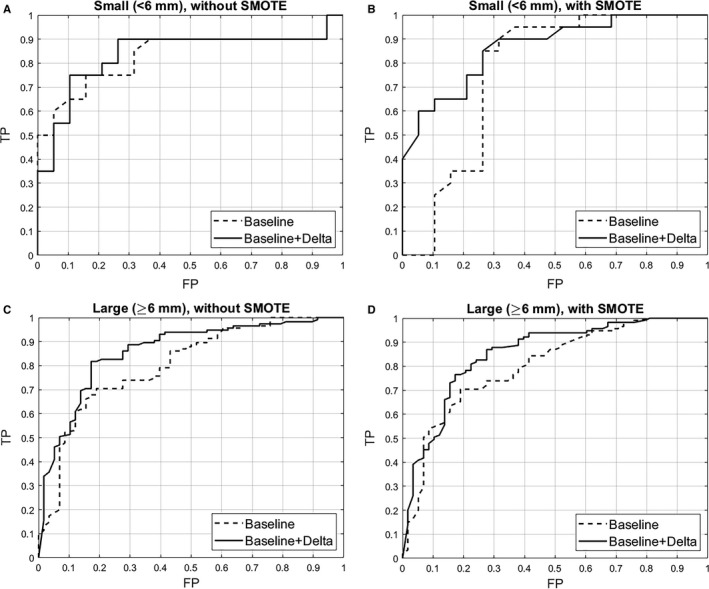
The final models revealed modest improvements for baseline and delta features when compared to only baseline features. The AUROCs for small- and intermediate-sized nodules were 0.83 (95% CI 0.76-0.90) and 0.76 (95% CI 0.71-0.81) for baseline-only radiomic features, respectively, and 0.84 (95% CI 0.77-0.90) and 0.84 (95% CI 0.80-0.88) for baseline and delta features, respectively. When intermediate and large nodules were combined, the AUROC for baseline-only features was 0.80 (95% CI 0.76-0.84) compared with 0.86 (95% CI 0.83-0.89) for baseline and delta features.
We found modest improvements in predicting lung cancer incidence by combining baseline and delta radiomics. Radiomics could be used to improve current size-based screening guidelines.
目前的肺癌筛查指南将阳性扫描阈值提高到最长直径 6 毫米。我们从基线和随访筛查中提取了放射组学特征,并使用三个结节大小类别(<6 毫米[小]、6-16 毫米[中]和≥16 毫米[大])进行了特定大小的分析,以预测肺癌的发病率。
我们从基线(T0)结节中提取了 219 个特征,并从 T0 到第一次随访(T1)提取了 219 个差值特征。为 160 例在 T1 或第二次随访筛查(T2)时被诊断为肺癌的病例和 307 例经三次连续阳性筛查且未被诊断为肺癌的结节阳性对照提取了结节。病例和对照组被分为训练和测试队列;使用分类器模型来识别最具预测性的特征。
与仅基线特征相比,基线和差值特征的最终模型显示出了适度的改进。小和中结节的基线特征的 AUROC 分别为 0.83(95%CI 0.76-0.90)和 0.76(95%CI 0.71-0.81),而基线和差值特征的 AUROC 分别为 0.84(95%CI 0.77-0.90)和 0.84(95%CI 0.80-0.88)。当将中等和大结节合并时,仅基线特征的 AUROC 为 0.80(95%CI 0.76-0.84),而基线和差值特征的 AUROC 为 0.86(95%CI 0.83-0.89)。
我们发现通过结合基线和差值放射组学,在预测肺癌发病率方面有适度的提高。放射组学可用于改进当前基于大小的筛查指南。