Mizuno Katsuhiro, Abe Takayuki, Ushiba Junichi, Kawakami Michiyuki, Ohwa Tomomi, Hagimura Kazuto, Ogura Miho, Okuyama Kohei, Fujiwara Toshiyuki, Liu Meigen
Department of Rehabilitation Medicine, Keio University School of Medicine, Tokyo, Japan.
School of Data Science, Yokohama City University, Yokohama, Japan.
JMIR Res Protoc. 2018 Dec 6;7(12):e12339. doi: 10.2196/12339.
We developed a brain-machine interface (BMI) system for poststroke patients with severe hemiplegia to detect event-related desynchronization (ERD) on scalp electroencephalogram (EEG) and to operate a motor-driven hand orthosis combined with neuromuscular electrical stimulation. ERD arises when the excitability of the ipsi-lesional sensorimotor cortex increases.
The aim of this study was to evaluate our hypothesis that motor training using this BMI system could improve severe hemiparesis that is resistant to improvement by conventional rehabilitation. We, therefore, planned and implemented a randomized controlled clinical trial (RCT) to evaluate the effectiveness and safety of intensive rehabilitation using the BMI system.
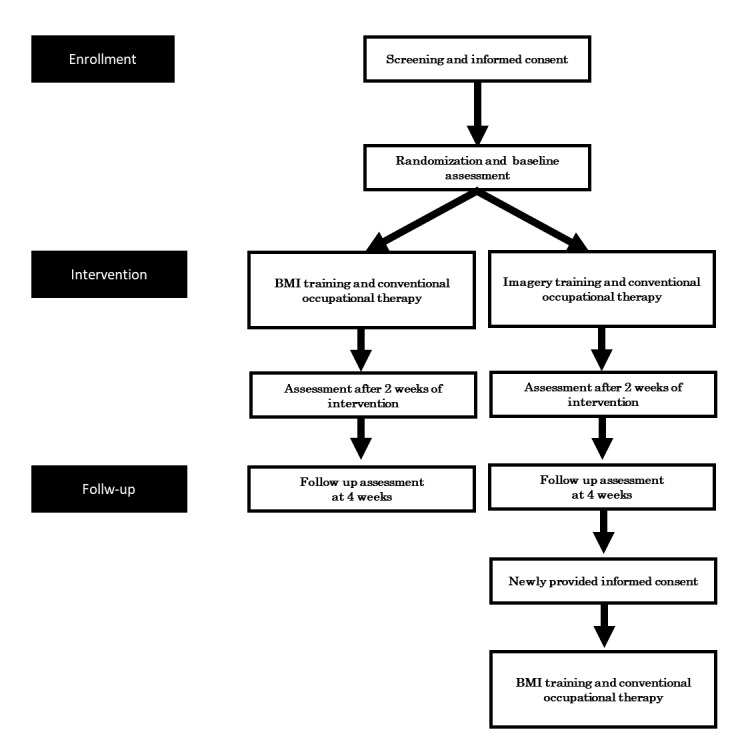
We conducted a single blind, multicenter RCT and recruited chronic poststroke patients with severe hemiparesis more than 90 days after onset (N=40). Participants were randomly allocated to the BMI group (n=20) or the control group (n=20). Patients in the BMI group repeated 10-second motor attempts to operate EEG-BMI 40 min every day followed by 40 min of conventional occupational therapy. The interventions were repeated 10 times in 2 weeks. Control participants performed a simple motor imagery without servo-action of the orthosis, and electrostimulation was given for 10 seconds for 40 min, similar to the BMI intervention. Overall, 40 min of conventional occupational therapy was also given every day after the control intervention, which was also repeated 10 times in 2 weeks. Motor functions and electrophysiological phenotypes of the paretic hands were characterized before (baseline), immediately after (post), and 4 weeks after (follow-up) the intervention. Improvement in the upper extremity score of the Fugl-Meyer assessment between baseline and follow-up was the main outcome of this study.
Recruitment started in March 2017 and ended in July 2018. This trial is currently in the data correcting phase. This RCT is expected to be completed by October 31, 2018.
No widely accepted intervention has been established to improve finger function of chronic poststroke patients with severe hemiparesis. The results of this study will provide clinical data for regulatory approval and novel, important understanding of the role of sensory-motor feedback based on BMI to induce neural plasticity and motor recovery.
UMIN Clinical Trials Registry UMIN000026372; https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi? recptno=R000030299 (Archived by WebCite at http://www.webcitation.org/743zBJj3D).
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): DERR1-10.2196/12339.
我们为患有严重偏瘫的中风后患者开发了一种脑机接口(BMI)系统,用于检测头皮脑电图(EEG)上的事件相关去同步化(ERD),并操作结合了神经肌肉电刺激的电动手部矫形器。当患侧感觉运动皮层的兴奋性增加时会出现ERD。
本研究的目的是评估我们的假设,即使用该BMI系统进行运动训练可以改善对传统康复治疗无反应的严重偏瘫。因此,我们计划并实施了一项随机对照临床试验(RCT),以评估使用BMI系统进行强化康复治疗的有效性和安全性。
我们进行了一项单盲、多中心RCT,招募了发病90天以上的慢性中风后严重偏瘫患者(N = 40)。参与者被随机分配到BMI组(n = 20)或对照组(n = 20)。BMI组的患者每天重复10秒的运动尝试以操作EEG-BMI,持续40分钟,随后进行40分钟的传统职业治疗。干预措施在2周内重复10次。对照组参与者进行简单的运动想象,不进行矫形器的伺服动作,并给予10秒的电刺激,持续40分钟,类似于BMI干预。总体而言,对照组干预后每天也给予40分钟的传统职业治疗,同样在2周内重复10次。在干预前(基线)、干预后立即(术后)和干预后4周(随访)对患侧手的运动功能和电生理表型进行了表征。本研究的主要结果是Fugl-Meyer评估中基线和随访之间上肢评分的改善。
招募工作于2017年3月开始,2018年7月结束。该试验目前处于数据校正阶段。预计该RCT将于2018年10月31日完成。
目前尚未建立被广泛接受的干预措施来改善患有严重偏瘫的慢性中风后患者的手指功能。本研究结果将为监管批准提供临床数据,并为基于BMI的感觉运动反馈在诱导神经可塑性和运动恢复中的作用提供新的重要认识。
UMIN临床试验注册中心UMIN000026372;https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000030299(由WebCite存档于http://www.webcitation.org/743zBJj3D)。
国际注册报告识别码(IRRID):DERR1-10.2.196/12339。