Division of Nephrology and Hypertension, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio; Departments of.
Pediatrics.
Clin J Am Soc Nephrol. 2019 Jan 7;14(1):57-65. doi: 10.2215/CJN.05890518. Epub 2018 Dec 6.
Kidney biopsy is an essential tool for the diagnosis and treatment of patients with kidney disease; however, because of its invasive nature, bleeding complications may arise.
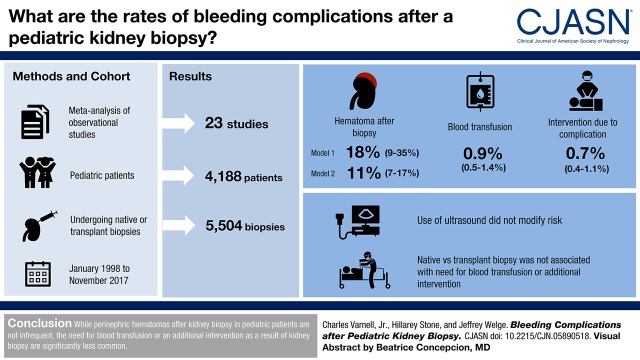
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We performed a meta-analysis of prospective or retrospective observational studies and randomized, controlled trials in pediatric patients undergoing native or transplant kidney biopsy in an inpatient or outpatient setting in MEDLINE-indexed studies from January 1998 to November 1, 2017 to determine the proportion of patients who develop hematoma, need blood transfusion, or need an additional intervention due to a complication after kidney biopsy.
Twenty-three studies of 5504 biopsies met inclusion criteria. The proportion of patients developing hematoma after biopsy was between 11% (95% confidence interval, 7% to 17%) and 18% (95% confidence interval, 9% to 35%) using two analyses that included different time periods. The proportion needing blood transfusion was 0.9% (95% confidence interval, 0.5% to 1.4%). The proportion needing an additional intervention due to postbiopsy complication was 0.7% (95% confidence interval, 0.4% to 1.1%). Secondary analysis was not possible due to lack of data in the original manuscripts on laboratory values, needle gauges, number of needle passes, age of patient, or performer (attending versus trainee). Analysis with metaregression found that use of real-time ultrasound during biopsy did not modify the risk for hematoma, requirement of a blood products transfusion, or requirement of an additional procedure after biopsy. Analysis with metaregression comparing native biopsies with transplant biopsies did not reveal that biopsy type (native kidney biopsy versus transplant kidney biopsy) was associated with the need for a blood transfusion or requirement of an additional intervention after biopsy.
The development of perinephric hematoma after kidney biopsy is not an infrequent finding. The proportion of patients requiring blood transfusion or needing an additional intervention as a result of kidney biopsy in pediatric patients is significantly smaller.
肾活检是诊断和治疗肾脏疾病患者的重要手段;然而,由于其侵袭性,可能会出现出血并发症。
设计、设置、参与者和测量方法:我们对 1998 年 1 月至 2017 年 11 月 1 日期间 MEDLINE 索引研究中接受住院或门诊治疗的原发性或移植肾活检的儿科患者进行了前瞻性或回顾性观察性研究和随机对照试验的荟萃分析,以确定发生血肿、需要输血或因肾活检后并发症需要进一步干预的患者比例。
23 项研究共 5504 例活检符合纳入标准。使用两种分析方法,包括不同时间段,活检后发生血肿的患者比例在 11%(95%置信区间,7%至 17%)和 18%(95%置信区间,9%至 35%)之间。需要输血的比例为 0.9%(95%置信区间,0.5%至 1.4%)。因活检后并发症需要进一步干预的比例为 0.7%(95%置信区间,0.4%至 1.1%)。由于原始手稿中缺乏关于实验室值、针规、针数、患者年龄或操作者(主治医生与受训者)的数据,因此无法进行二次分析。荟萃回归分析发现,活检过程中使用实时超声并不能改变血肿、血液制品输血或活检后需要进行额外手术的风险。荟萃回归分析比较原发性肾活检与移植肾活检,未发现活检类型(原发性肾活检与移植肾活检)与输血或活检后需要进一步干预相关。
肾活检后肾周血肿的发生并不少见。儿科患者因肾活检需要输血或需要进一步干预的比例明显较小。