Eberlin Kyle R, Ducic Ivica
Department of Surgery Division of Plastic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, Mass.
Washington Nerve Institute, McLean, Va.
Plast Reconstr Surg Glob Open. 2018 Oct 16;6(10):e1952. doi: 10.1097/GOX.0000000000001952. eCollection 2018 Oct.
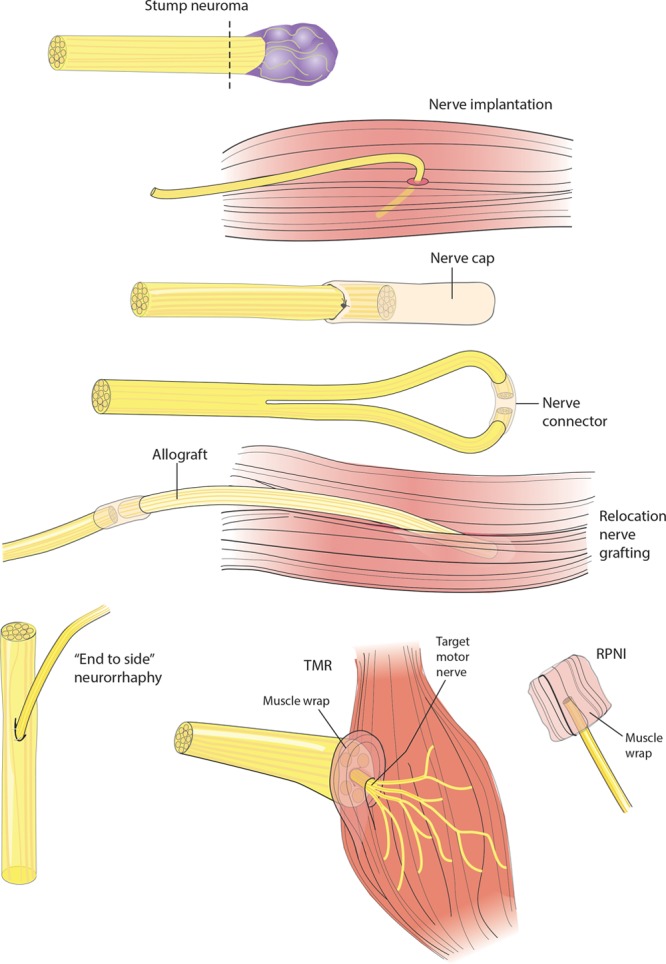
Successful treatment of the painful neuroma is a particular challenge to the nerve surgeon. Historically, symptomatic neuromas have primarily been treated with excision and implantation techniques, which are inherently passive and do not address the terminal end of the nerve. Over the past decade, the surgical management of neuromas has undergone a paradigm shift synchronous with the development of contemporary techniques aiming to satisfy the nerve end. In this article, we describe the important features of surgical treatment, including the approach to diagnosis with consideration of neuroma type and the decision of partial versus complete neuroma excision. A comprehensive list of the available surgical techniques for management following neuroma excision is presented, the choice of which is often predicated upon the availability of the terminal nerve end for reconstruction. Techniques for neuroma reconstruction in the presence of an intact terminal nerve end include hollow tube reconstruction and auto- or allograft nerve reconstruction. Techniques for neuroma management in the absence of an intact or identifiable terminal nerve end include submuscular or interosseous implantation, centro-central neurorrhaphy, relocation nerve grafting, nerve cap placement, use of regenerative peripheral nerve interface, "end-to-side" neurorrhaphy, and targeted muscle reinnervation. These techniques can be further categorized into passive/ablative and active/reconstructive modalities. The nerve surgeon must be aware of available treatment options and should carefully choose the most appropriate intervention for each patient. Comparative studies are lacking and will be necessary in the future to determine the relative effectiveness of each technique.
成功治疗疼痛性神经瘤对神经外科医生来说是一项特殊挑战。从历史上看,有症状的神经瘤主要采用切除和植入技术进行治疗,这些技术本质上是被动的,并未处理神经的末端。在过去十年中,神经瘤的外科治疗管理与旨在满足神经末端的当代技术发展同步发生了范式转变。在本文中,我们描述了手术治疗的重要特征,包括考虑神经瘤类型的诊断方法以及部分与完全神经瘤切除的决策。列出了神经瘤切除后可用的手术管理技术的综合清单,其选择通常取决于用于重建的末端神经的可用性。在存在完整末端神经的情况下进行神经瘤重建的技术包括空心管重建和自体或异体神经移植重建。在没有完整或可识别的末端神经的情况下进行神经瘤管理的技术包括肌下或骨间植入、中央对中央神经缝合、重新定位神经移植、神经帽放置、使用再生周围神经接口、“端对侧”神经缝合和靶向肌肉再支配。这些技术可进一步分为被动/消融和主动/重建方式。神经外科医生必须了解可用的治疗选择,并应为每位患者仔细选择最合适的干预措施。目前缺乏比较研究,未来有必要进行比较研究以确定每种技术的相对有效性。