Kim Ko Eun, Yang Pil Sung, Jang Eunsun, Kim Sungjin, Joung Boyoung
Department of Ophthalmology, Nowon Eulji Medical Center, Eulji University, Seoul, Korea.
Department of Cardiology, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
Yonsei Med J. 2019 Jan;60(1):65-72. doi: 10.3349/ymj.2019.60.1.65.
Antithrombotic therapy could be related with nuisance bleeding. This study investigated whether vitreous hemorrhage (VH) is associated with specific types of antithrombotic medication in patients with atrial fibrillation (AF).
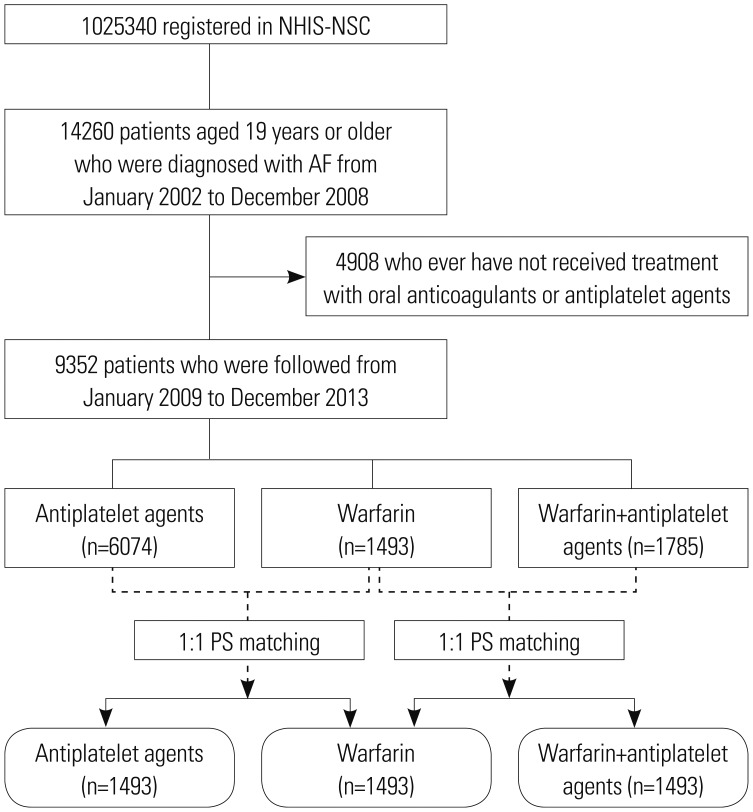
In the Korean National Health Insurance Service National Sample Cohort, we identified 9352 antiplatelet/anticoagulant-treated AF patients. The occurrence of VH was compared between warfarin (n=1493) and a propensity score (PS)-matched antiplatelet group (n=1493) and between warfarin (n=1493) and a PS-matched warfarin+antiplatelet group (n=1493).
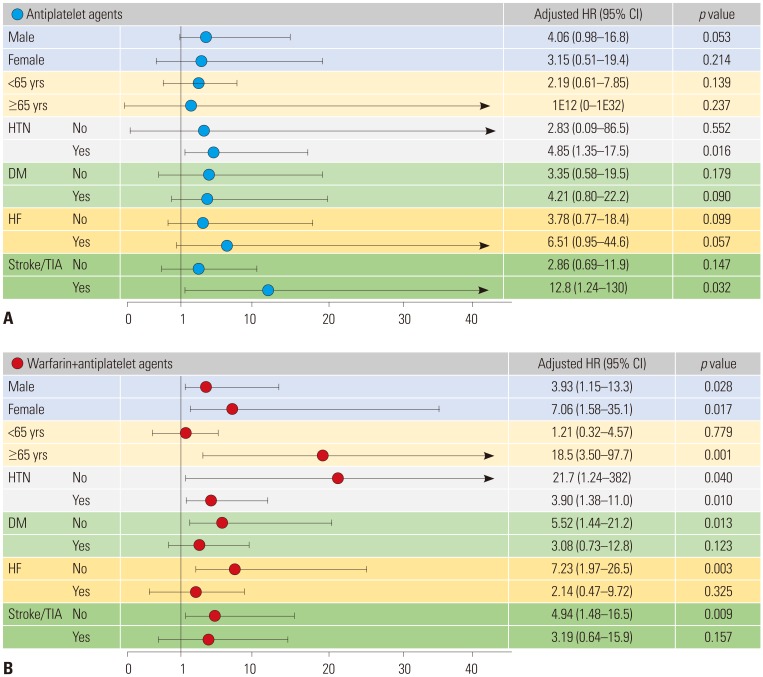
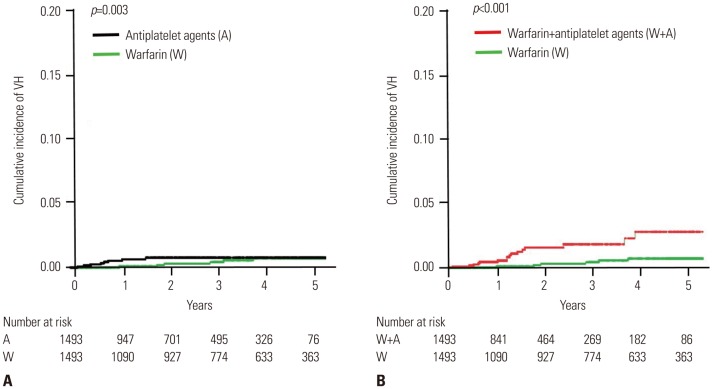
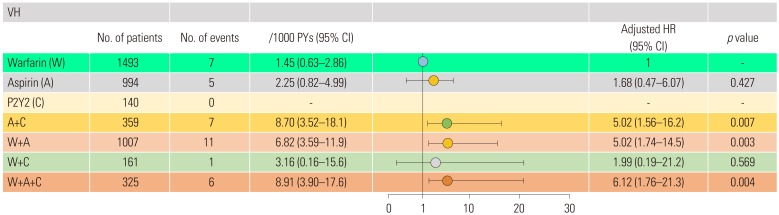
The outcomes of VH were lower in the warfarin than in the matched antiplatelet (1.45 vs. 3.72 events/1000 patient-years) and matched warfarin+antiplatelet groups (1.45 vs. 6.87 events/1000 patient-years). Compared with warfarin, the risk of VH increased with antiplatelet [adjusted hazard ratio (aHR) 3.90; 95% confidence interval (CI) 1.22-12.4, =0.022] and warfarin+antiplatelet agents (aHR 4.39, 95% CI 1.74-11.2, =0.002). Compared with warfarin only, warfarin+antiplatelet agents increased the risk of VH in patients ≥65 years, regardless of gender and hypertension. The risk of VH was significantly higher with dual antiplatelet therapy (aHR: 5.02, 95% CI: 1.56-16.2, =0.007) or in dual (aHR: 5.02, 95% CI: 1.74-14.5, =0.003) or triple therapy using warfarin and antiplatelet agents than with warfarin monotherapy (aHR: 6.12, 95% CI: 1.76-21.3, =0.004).
Dual antiplatelet or triple therapy increased the risk of VH significantly, compared to warfarin monotherapy. Considering the low efficacy of preventing ischemic stroke and high risk of bleeding, dual or triple therapy using warfarin and antiplatelet agents should be avoided to prevent VH in AF patients.
抗血栓治疗可能与烦扰性出血有关。本研究调查了心房颤动(AF)患者的玻璃体积血(VH)是否与特定类型的抗血栓药物相关。
在韩国国民健康保险服务国家样本队列中,我们确定了9352例接受抗血小板/抗凝治疗的AF患者。比较了华法林组(n = 1493)与倾向评分(PS)匹配的抗血小板组(n = 1493)之间以及华法林组(n = 1493)与PS匹配的华法林+抗血小板组(n = 1493)之间VH的发生率。
华法林组VH的发生率低于匹配的抗血小板组(1.45对3.72事件/1000患者年)和匹配的华法林+抗血小板组(1.45对6.87事件/1000患者年)。与华法林相比,抗血小板药物(调整后风险比[aHR] 3.90;95%置信区间[CI] 1.22 - 12.4,P = 0.022)和华法林+抗血小板药物(aHR 4.39,95% CI 1.74 - 11.2,P = 0.002)使VH风险增加。与仅使用华法林相比,华法林+抗血小板药物在≥65岁患者中增加了VH风险,无论性别和是否患有高血压。双联抗血小板治疗(aHR:5.02,95% CI:1.56 - 16.2,P = 0.007)或使用华法林和抗血小板药物的双联(aHR:5.02,95% CI:1.74 - 14.5,P = 0.003)或三联治疗中VH风险显著高于华法林单药治疗(aHR:6.12,95% CI:1.76 - 21.3,P = 0.004)。
与华法林单药治疗相比,双联抗血小板或三联治疗显著增加了VH风险。考虑到预防缺血性卒中的疗效低且出血风险高,应避免使用华法林和抗血小板药物的双联或三联治疗以预防AF患者的VH。