1 The Department of Medicine/Division of Cardiology and Center for Cardiovascular Diseases & Sciences Louisiana State University Health Sciences Center-Shreveport (LSUHSC-S) Shreveport LA.
J Am Heart Assoc. 2018 Nov 20;7(22):e010156. doi: 10.1161/JAHA.118.010156.
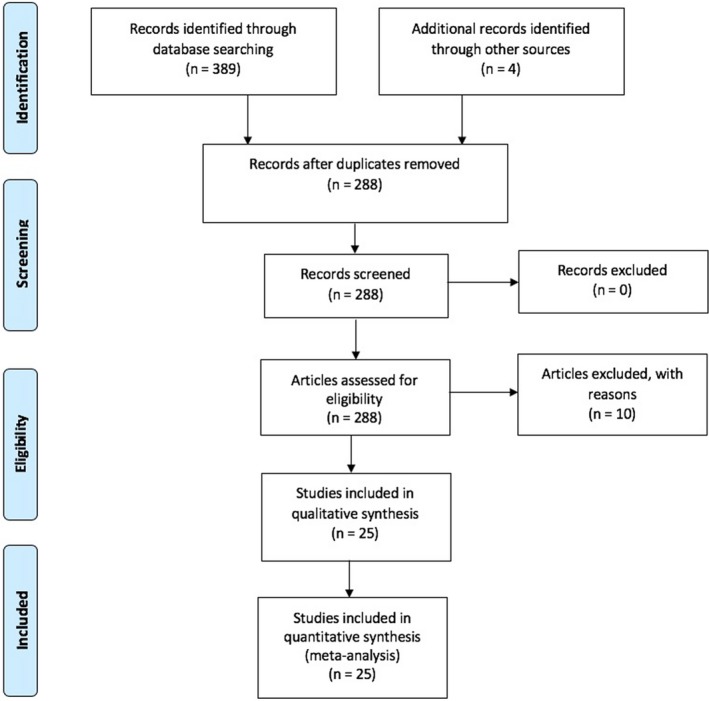
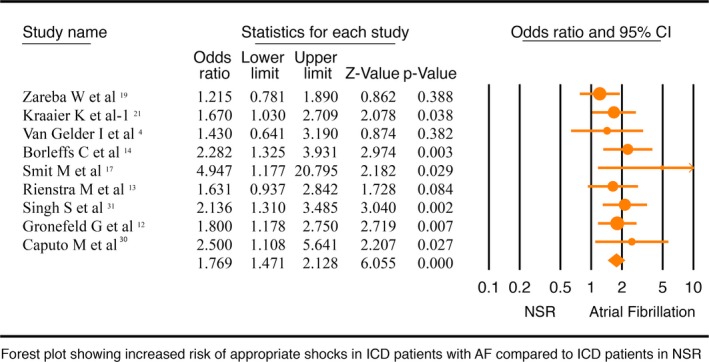
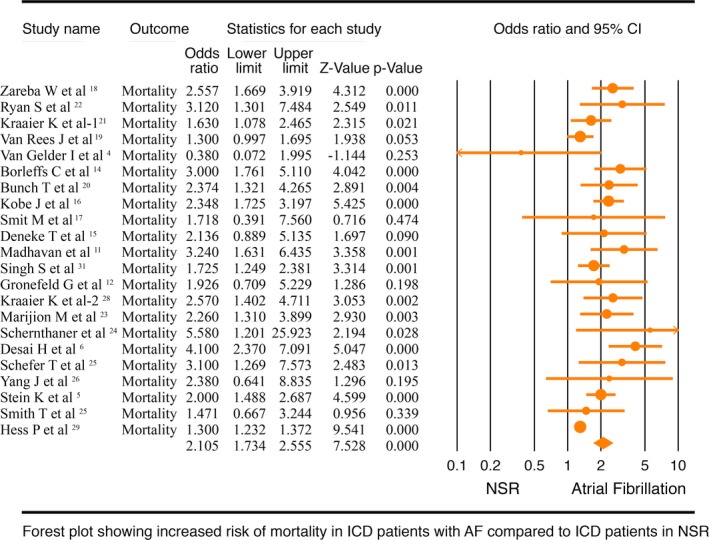
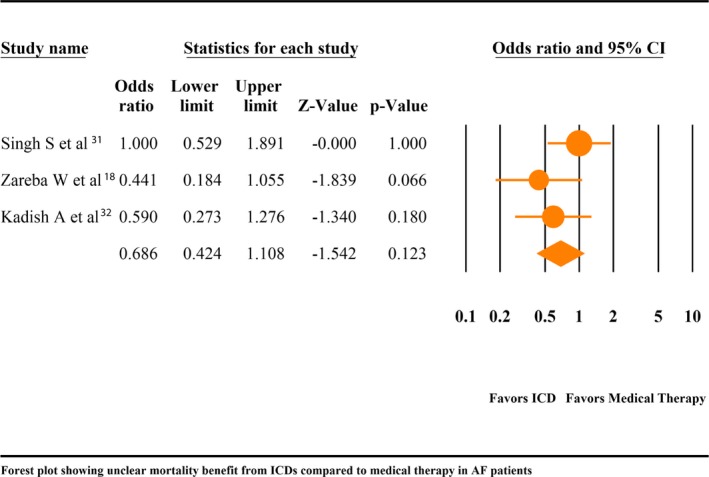
Background Implantable cardioverter-defibrillator ( ICD ) improves survival when used for primary or secondary prevention of sudden cardiac death. Whether the benefits of ICD in patients with atrial fibrillation ( AF) are similar to those with normal sinus rhythm ( NSR ) is not well established. The aim of this study is to investigate whether ICD patients with AF are at higher risk of mortality and appropriate shock therapy compared with patients with NSR . Methods and Results Literature was searched and 25 observational studies with 63 283 patients were included in this meta-analysis. We compared the outcomes of (1) all-cause mortality and appropriate shock therapy among AF and NSR patients who received ICD for either primary or secondary prevention and (2) all-cause mortality among AF patients with ICD versus guideline directed medical therapy. All-cause mortality (odds ratio, 2.11; 95% confidence interval, 1.73-2.56; P<0.001) and incidence of appropriate shock therapy (odds ratio, 1.77; 95% confidence interval, 1.47-2.13; P<0.001) were significantly higher in ICD patients with AF as compared to NSR . There was no statistically significant mortality benefit from ICD compared with medical therapy in AF patients (odds ratio, 0.69; 95% confidence interval, 0.42-1.11; P=0.12) based on a separate meta-analysis of 3 studies with 387 patients. Conclusions Overall mortality and appropriate shock therapy are higher in ICD patients with AF as compared with NSR . The impact of ICD on all-cause mortality in AF patients when compared to goal-directed medical therapy is unclear, and randomized controlled trials are needed comparing AF patients with ICD and those who have indications for ICD, but are only on medical therapy.
背景 植入式心脏复律除颤器(ICD)可提高因心脏性猝死进行一级或二级预防患者的生存率。但尚不清楚 AF 患者使用 ICD 的获益是否与窦性心律(NSR)患者相同。本研究旨在调查 AF 患者 ICD 治疗后死亡率和恰当电击治疗风险是否高于 NSR 患者。
方法和结果 文献检索,纳入 25 项观察性研究共 63283 例患者进行 meta 分析。比较了(1)因一级或二级预防目的植入 ICD 的 AF 和 NSR 患者的全因死亡率和恰当电击治疗情况,(2)植入 ICD 的 AF 患者与指南指导的药物治疗的全因死亡率。与 NSR 患者相比,AF 患者 ICD 治疗的全因死亡率(优势比,2.11;95%置信区间,1.73-2.56;P<0.001)和恰当电击治疗发生率(优势比,1.77;95%置信区间,1.47-2.13;P<0.001)均显著更高。但基于 3 项研究共 387 例患者的单独 meta 分析,AF 患者 ICD 治疗与药物治疗比较并未显著降低死亡率(优势比,0.69;95%置信区间,0.42-1.11;P=0.12)。
结论 与 NSR 患者相比,AF 患者 ICD 治疗的总体死亡率和恰当电击治疗更高。但与药物治疗相比,AF 患者 ICD 治疗对全因死亡率的影响尚不清楚,需要比较 AF 患者和有 ICD 指征但仅接受药物治疗的患者的随机对照试验。