Sakr Yasser, Jaschinski Ulrich, Wittebole Xavier, Szakmany Tamas, Lipman Jeffrey, Ñamendys-Silva Silvio A, Martin-Loeches Ignacio, Leone Marc, Lupu Mary-Nicoleta, Vincent Jean-Louis
Department of Anaesthesiology and Intensive Care, Uniklinikum Jena, Germany.
Klinik für Anästhesiologie und Operative Intensivmedizin, Klinikum Augsburg, Germany.
Open Forum Infect Dis. 2018 Nov 19;5(12):ofy313. doi: 10.1093/ofid/ofy313. eCollection 2018 Dec.
There is a need to better define the epidemiology of sepsis in intensive care units (ICUs) around the globe.
The Intensive Care over Nations (ICON) audit prospectively collected data on all adult (>16 years) patients admitted to the ICU between May 8 and May 18, 2012, except those admitted for less than 24 hours for routine postoperative surveillance. Data were collected daily for a maximum of 28 days in the ICU, and patients were followed up for outcome data until death, hospital discharge, or for 60 days. Participation was entirely voluntary.
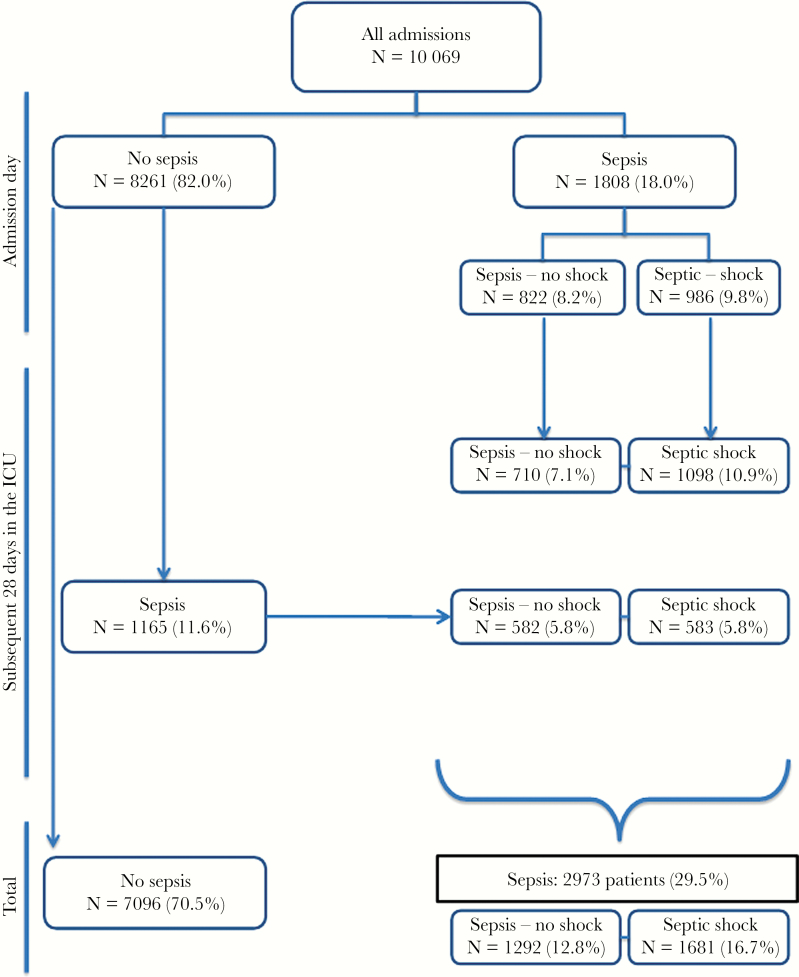
The audit included 10069 patients from Europe (54.1%), Asia (19.2%), America (17.1%), and other continents (9.6%). Sepsis, defined as infection with associated organ failure, was identified during the ICU stay in 2973 (29.5%) patients, including in 1808 (18.0%) already at ICU admission. Occurrence rates of sepsis varied from 13.6% to 39.3% in the different regions. Overall ICU and hospital mortality rates were 25.8% and 35.3%, respectively, in patients with sepsis, but it varied from 11.9% and 19.3% (Oceania) to 39.5% and 47.2% (Africa), respectively. After adjustment for possible confounders in a multilevel analysis, independent risk factors for in-hospital death included older age, higher simplified acute physiology II score, comorbid cancer, chronic heart failure (New York Heart Association Classification III/IV), cirrhosis, use of mechanical ventilation or renal replacement therapy, and infection with spp.
Sepsis remains a major health problem in ICU patients worldwide and is associated with high mortality rates. However, there is wide variability in the sepsis rate and outcomes in ICU patients around the globe.
有必要更好地界定全球重症监护病房(ICU)中脓毒症的流行病学特征。
“跨国重症监护(ICON)”审计前瞻性收集了2012年5月8日至5月18日期间入住ICU的所有成年(>16岁)患者的数据,但因常规术后监测入院不足24小时的患者除外。在ICU中,每天收集数据,最长收集28天,并对患者进行随访以获取结局数据,直至死亡、出院或随访60天。参与完全是自愿的。
该审计纳入了来自欧洲(54.1%)、亚洲(19.2%)、美洲(17.1%)和其他各大洲(9.6%)的10069例患者。脓毒症定义为伴有相关器官功能衰竭的感染,在ICU住院期间,2973例(29.5%)患者被确诊为脓毒症,其中1808例(18.0%)在入住ICU时就已确诊。不同地区脓毒症的发生率从13.6%到39.3%不等。脓毒症患者的ICU总体死亡率和医院死亡率分别为25.8%和35.3%,但在不同地区有所不同,大洋洲分别为11.9%和19.3%,非洲分别为39.5%和47.2%。在多水平分析中对可能的混杂因素进行校正后,院内死亡的独立危险因素包括年龄较大、简化急性生理学II评分较高、合并癌症、慢性心力衰竭(纽约心脏协会分级III/IV级)、肝硬化、使用机械通气或肾脏替代治疗以及感染 菌。
脓毒症仍是全球ICU患者面临的主要健康问题,且与高死亡率相关。然而,全球ICU患者的脓毒症发生率和结局存在很大差异。