Udeh Chiedozie I, You Jing, Wanek Matthew R, Dalton Jarrod, Udeh Belinda L, Demirjian Sevag, Rahman Nadeem, Hata J Steven
Center for Critical Medicine, Anesthesiology Institute, 9500 Euclid Avenue, (J4-331), Cleveland, OH 44195 USA.
Department of Special Line Product Development, Progressive Insurance, 300 N. Commons Blvd, Cleveland, OH 44143 USA.
Perioper Med (Lond). 2018 Dec 14;7:29. doi: 10.1186/s13741-018-0110-y. eCollection 2018.
The use of hyperoncotic albumin (HA) for shock resuscitation is controversial given concerns about its cost, effectiveness, and potential for nephrotoxicity. We evaluated the association between early exposure to hyperoncotic albumin (within the first 48 h of onset of shock) and acute organ dysfunction in post-surgical patients with shock.
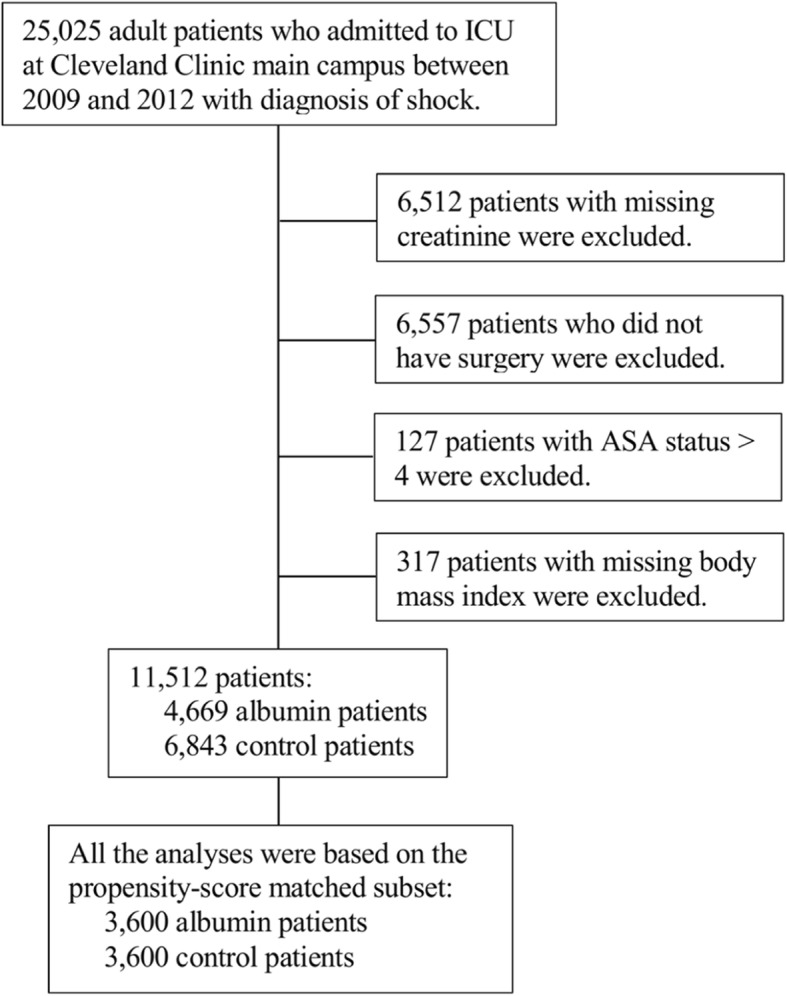
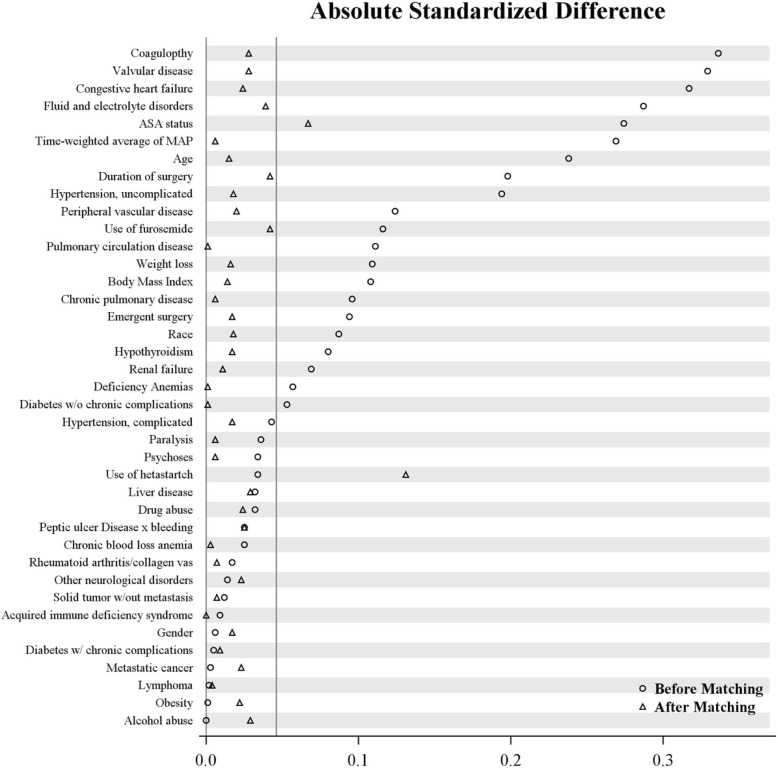
This retrospective, cohort study included 11,512 perioperative patients with shock from 2009 to 2012. Shock was defined as requirement for vasopressors to maintain adequate mean arterial pressure and/or elevated lactate (> 2.2 mmol/L). Subsets of 3600 were selected after propensity score and exact matching on demographics, comorbidities, and treatment variables (> 30). There was a preponderance of cardiac surgery patients. Proportional odds logistic regression, multivariable logistic regression or Cox proportional hazard regression models measured association between hyperoncotic albumin and acute kidney injury (AKI), hepatic injury, ICU days, and mortality.
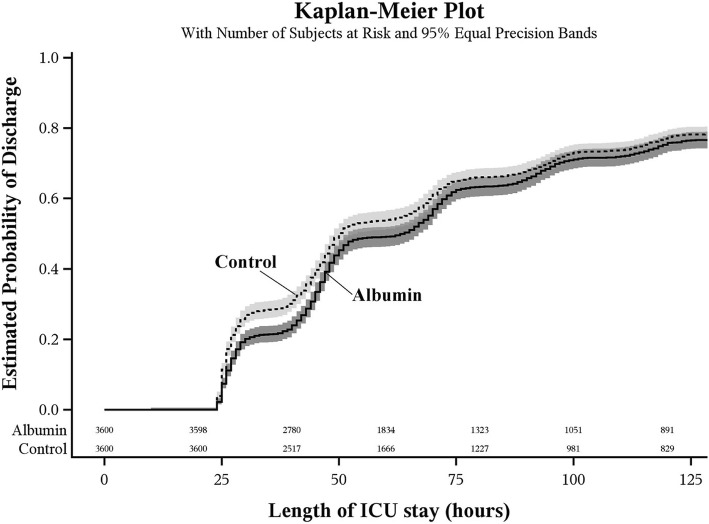
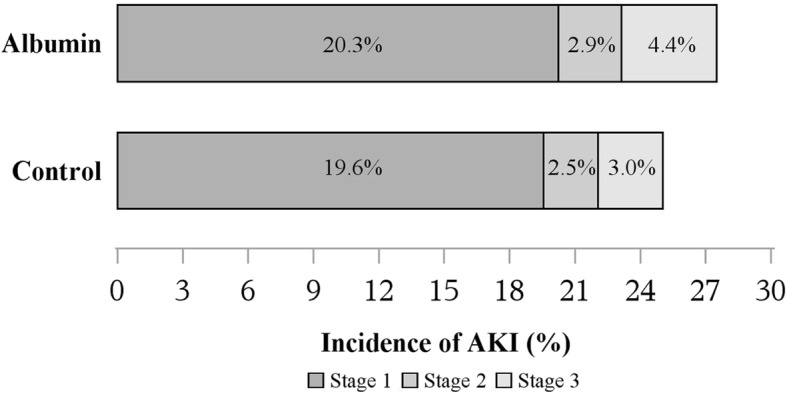
Hyperoncotic albumin-exposed patients showed greater risk of acute kidney injury compared to controls (OR 1.10, 95% CI 1.04, 1.17. = 0.002), after adjusting for imbalanced co-variables. Within matched patients, 20.3%, 2.9%, and 4.4% of HA patients experienced KDIGO stages 1-3 AKI, versus 19.6%, 2.5%, and 3.0% of controls. There was no difference in hepatic injury OR 1.16; 98.3% CI 0.85, 1.58); ICU days, (HR 1.05; 98.3% CI 1.00, 1.11); or mortality, (OR 0.88; 98.3% CI 0.64, 1.20).
Early exposure to hyperoncotic albumin in postoperative shock appeared to be associated with acute kidney injury. There did not appear to be any association with hepatic injury, mortality, or ICU days. The clinical and economic implications of this finding warrant further investigation.
鉴于对高渗白蛋白(HA)的成本、有效性及肾毒性可能性的担忧,其用于休克复苏存在争议。我们评估了术后休克患者早期暴露于高渗白蛋白(休克发作后48小时内)与急性器官功能障碍之间的关联。
这项回顾性队列研究纳入了2009年至2012年期间11512例围手术期休克患者。休克定义为需要使用血管升压药来维持足够的平均动脉压和/或乳酸水平升高(>2.2 mmol/L)。在倾向评分以及根据人口统计学、合并症和治疗变量(>30)进行精确匹配后,选取了3600例患者的子集。心脏手术患者占多数。比例优势逻辑回归、多变量逻辑回归或Cox比例风险回归模型用于衡量高渗白蛋白与急性肾损伤(AKI)、肝损伤、ICU住院天数和死亡率之间的关联。
在调整不平衡的协变量后,与对照组相比,暴露于高渗白蛋白的患者发生急性肾损伤的风险更高(OR 1.10,95%CI 1.04,1.17;P = 0.002)。在匹配患者中,20.3%、2.9%和4.4%的HA患者经历了KDIGO 1 - 3期AKI,而对照组分别为19.6%、2.5%和3.0%。肝损伤(OR 1.16;98.3%CI 0.85,1.58)、ICU住院天数(HR 1.05;98.3%CI 1.00,1.11)或死亡率(OR 0.88;98.3%CI 0.64,1.20)方面没有差异。
术后休克患者早期暴露于高渗白蛋白似乎与急性肾损伤有关。与肝损伤、死亡率或ICU住院天数似乎没有任何关联。这一发现的临床和经济意义值得进一步研究。