Department of Hepatobiliary & Pancreatic Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450000, Henan Province, China.
Department of Hepatobiliary & Pancreatic Surgery, The First Norman Bethune Hospital Affiliated to Jilin University, Changchun, 130021, Jilin Province, China.
Sci Rep. 2018 Dec 19;8(1):17979. doi: 10.1038/s41598-018-36365-5.
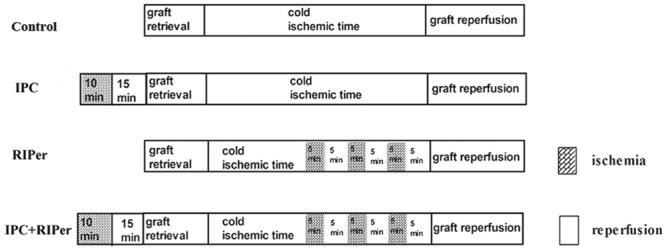
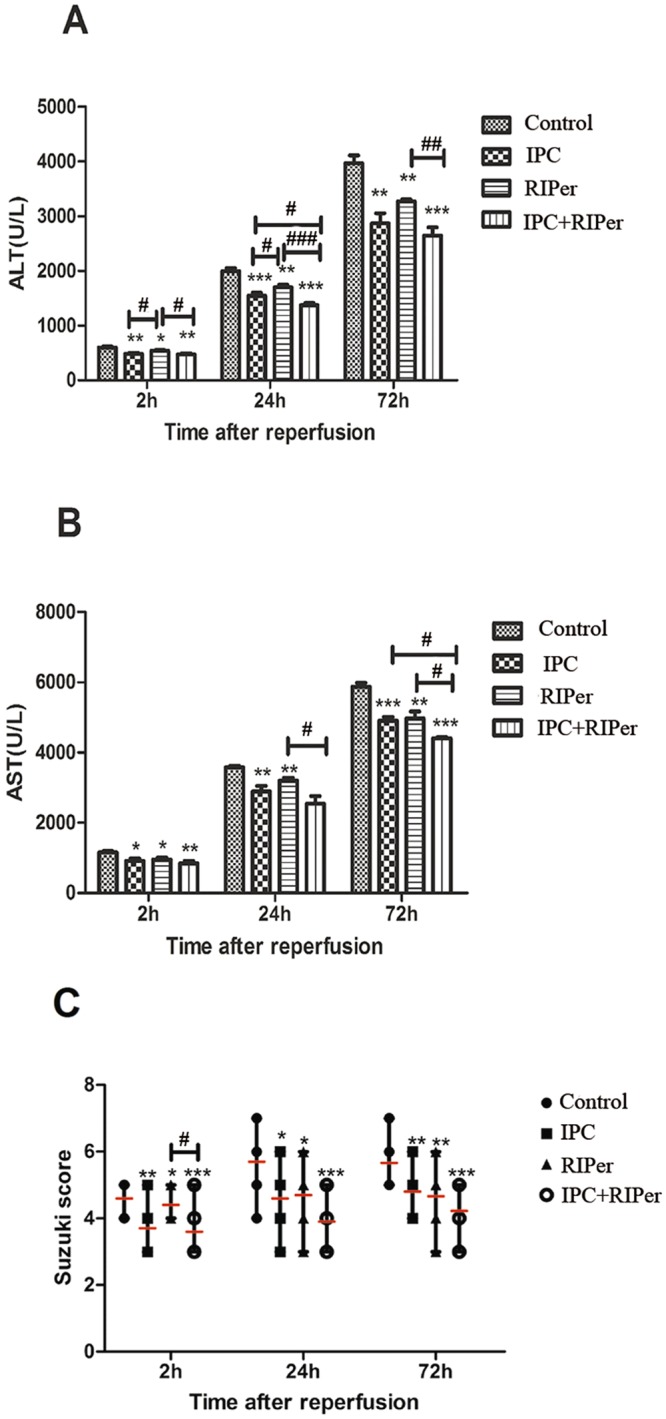
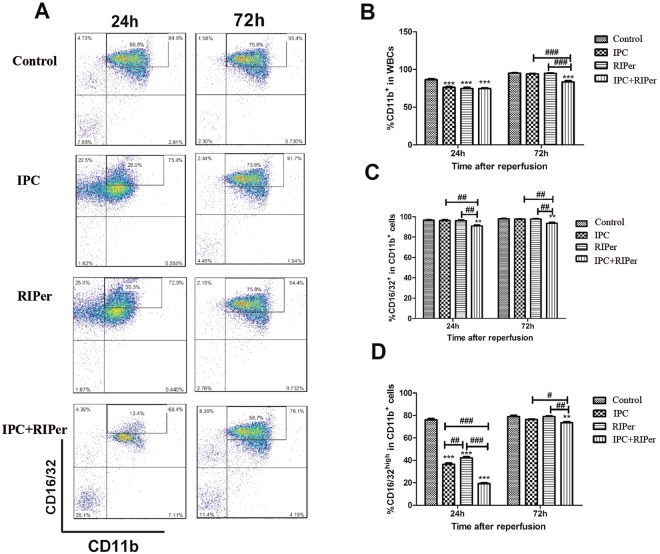
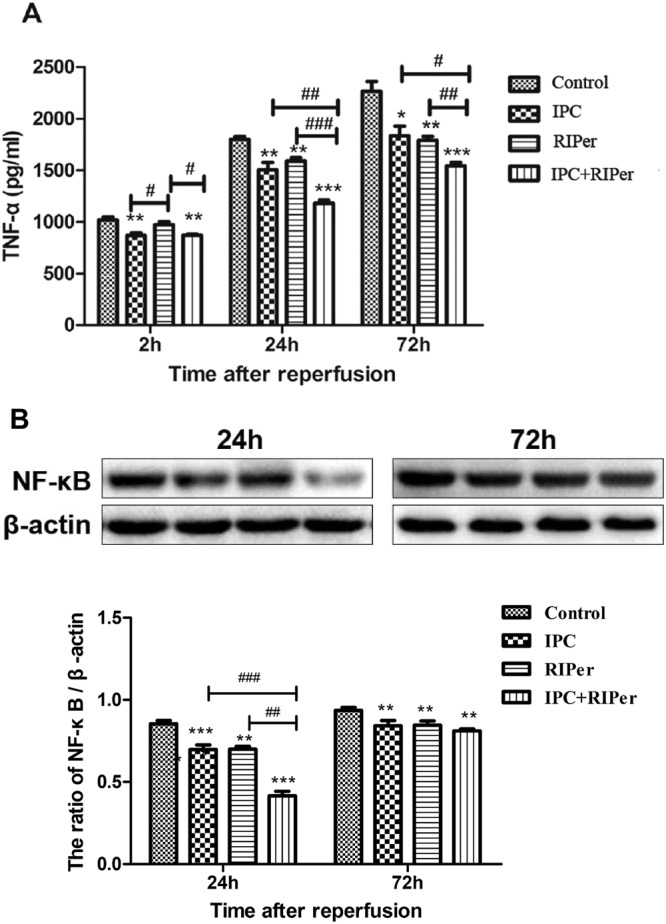
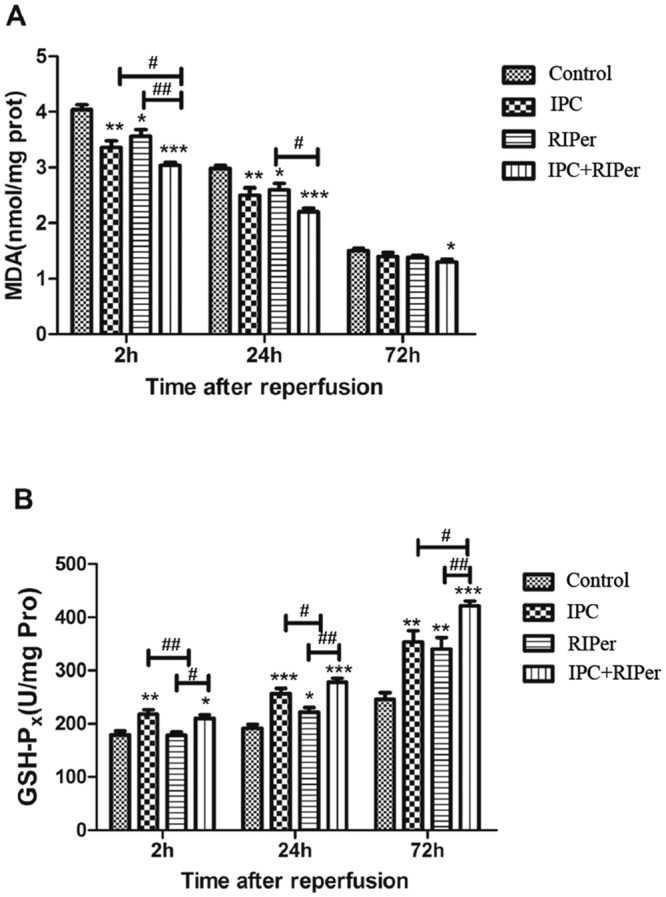
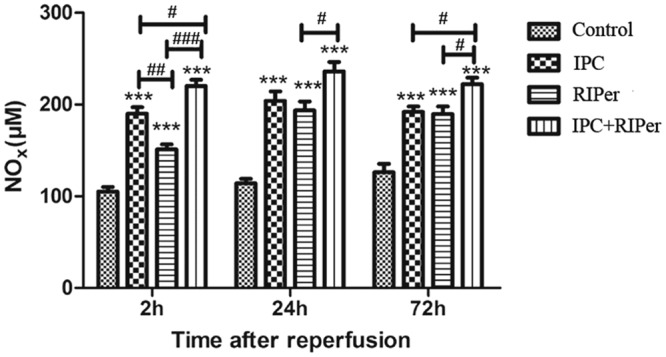
Ischemic preconditioning (IPC) and remote ischemic perconditioning (RIPer) confer protective effects against liver ischemia-reperfusion injury (IRI), but data about RIPer applying in liver transplantation is lacking. The study aimed to evaluate whether the combination of IPC and RIPer provides reinforced protective effects. C57BL/6 mice (160 pairs) were allocated into four groups: control, subjected to liver transplantation only; IPC, donor hilar was clamped for 10 min followed by 15 min of reperfusion; RIPer, three cycles of occlusion (5 min) and opening (5 min) of femoral vascular bundle were performed before reperfusion; IPC + RIPer, donors and recipients were subjected to IPC and RIPer respectively. Liver tissues were obtained for histological evaluation, TUNEL staining, malondialdehyde assays, GSH-Px assays, and NF-κB p65 protein and Bcl-2/Bax mRNA analyses. Blood samples were used to evaluate ALT, AST, TNF-α, NOx levels and flow cytometry. We found that protective efficacy of RIPer is less than IPC in terms of ALT, TNF-α, GSH-Px and NOx at 2 h postoperation, but almost equivalent at 24 h and 72 h postoperation. Except for Suzuki scores, ALT, Bcl-2/Bax mRNA ratio, other indices showed that combined treatment brought enhanced attenuation in IRI, compared with single treatment, through additive effects on antioxidation, anti-apoptosis, modulation of microcirculation disturbance, and inhibition of innate immune response. This study suggested a combined strategy that could enhance protection against IRI in clinical liver transplantation, otherwise, provided a hint that RIPer's mechanism might be partly or totally different from IPC in humoral pathway.
缺血预处理(IPC)和远程缺血预处理(RIPer)可减轻肝缺血再灌注损伤(IRI),但 RIPer 在肝移植中的应用数据尚缺乏。本研究旨在评估 IPC 与 RIPer 联合应用是否具有更强的保护作用。将 160 对 C57BL/6 小鼠分为四组:对照组,仅行肝移植;IPC 组,夹闭供肝肝门 10min 后再灌注 15min;RIPer 组,再灌注前进行 3 个循环的股血管束阻断(5min)和开放(5min);IPC+RIPer 组,供体和受体分别行 IPC 和 RIPer。取肝组织行组织学评估、TUNEL 染色、丙二醛测定、GSH-Px 测定、NF-κB p65 蛋白和 Bcl-2/BaxmRNA 分析。采集血样检测 ALT、AST、TNF-α、NOx 水平和流式细胞术。结果发现,与 IPC 相比,RIPer 在术后 2h 的 ALT、TNF-α、GSH-Px 和 NOx 水平较低,但在术后 24h 和 72h 时几乎相当。除 Suzuki 评分外,与单一处理相比,联合处理在 ALT、Bcl-2/BaxmRNA 比值等其他指标上通过抗氧化、抗凋亡、调节微循环紊乱和抑制固有免疫反应,增强了对 IRI 的衰减作用。该研究提示,联合策略可能增强临床肝移植中对 IRI 的保护作用,或者提示 RIPer 的作用机制在体液途径上可能部分或完全不同于 IPC。