Clinical Health Promotion Centre, WHO-CC, Bispebjerg and Frederiksberg Hospital, Copenhagen University Hospitals, Nordre Fasanvej 57, Build. 14, Entr. 5, 2nd fl, 2000, Frederiksberg, Denmark.
School of Medicine, National Yang-Ming University, Taipei, Taiwan.
Implement Sci. 2018 Dec 22;13(1):153. doi: 10.1186/s13012-018-0848-0.
Implementation of clinical health promotion (CHP) aiming at better health gain is slow despite its effect. CHP focuses on potentially modifiable lifestyle risks such as smoking, alcohol, diet, and physical inactivity. An operational program was created to improve implementation. It included patients, staff, and the organization, and it combined existing standards, indicators, documentation models, a performance recognition process, and a fast-track implementation model. The aim of this study was to evaluate if the operational program improved implementation of CHP in clinical hospital departments, as measured by health status of patients and staff, frequency of CHP service delivery, and standards compliance.
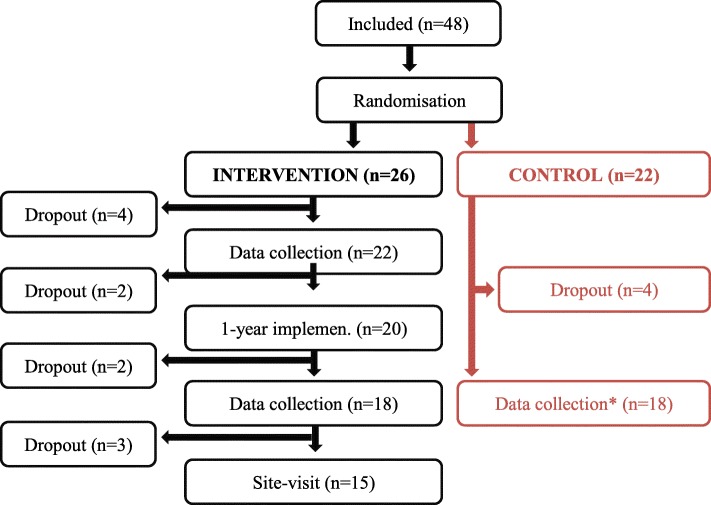
Forty-eight hospital departments were recruited via open call and stratified by country. Departments were assigned to the operational program (intervention) or usual routine (control group). Data for analyses included 36 of these departments and their 5285 patients (median 147 per department; range 29-201), 2529 staff members (70; 10-393), 1750 medical records (50; 50-50), and standards compliance assessments. Follow-up was measured after 1 year. The outcomes were health status, service delivery, and standards compliance.
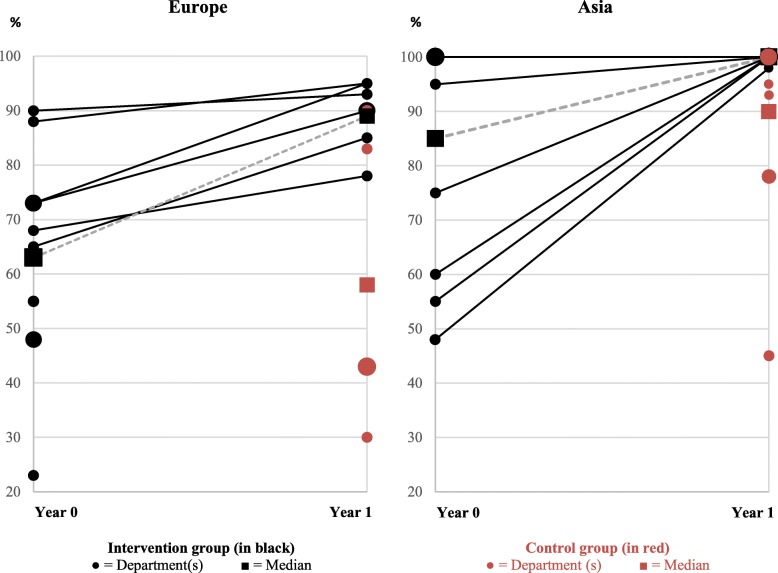
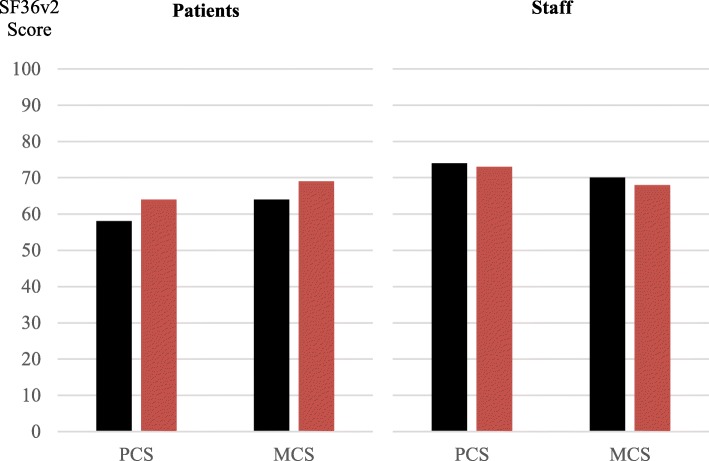
No health differences between groups were found, but the intervention group had higher identification of lifestyle risk (81% versus 60%, p < 0.01), related information/short intervention and intensive intervention (54% versus 39%, p < 0.01 and 43% versus 25%, p < 0.01, respectively), and standards compliance (95% versus 80%, p = 0.02).
The operational program improved implementation by way of lifestyle risk identification, CHP service delivery, and standards compliance. The unknown health effects, the bias, and the limitations should be considered in implementation efforts and further studies.
ClinicalTrials.gov : NCT01563575. Registered 27 March 2012. https://clinicaltrials.gov/ct2/show/NCT01563575.
尽管临床健康促进(CHP)具有积极作用,但实施进展仍然缓慢。CHP 专注于可改变的生活方式风险因素,如吸烟、饮酒、饮食和缺乏身体活动。为了提高实施效果,创建了一个操作性方案。该方案涵盖了患者、医护人员和组织,并整合了现有的标准、指标、文件模型、绩效认可流程和快速实施模式。本研究旨在评估该操作性方案是否能提高临床医院科室 CHP 的实施效果,评估指标包括患者和医护人员的健康状况、CHP 服务提供的频率以及标准执行情况。
通过公开招募和分层,从 48 个国家的医院科室中选取研究对象。科室被随机分配到操作性方案(干预组)或常规流程(对照组)中。数据分析纳入了 36 个科室及其 5285 名患者(科室中位数为 147 例,范围为 29-201 例)、2529 名医护人员(70 名,范围为 10-393 名)、1750 份病历(50 份,范围为 50-50 份)和标准执行情况评估。随访时间为 1 年后。评估指标包括健康状况、服务提供和标准执行情况。
组间健康状况无显著差异,但干预组在生活方式风险识别(81%比 60%,p<0.01)、相关信息/短期干预和强化干预(54%比 39%,p<0.01 和 43%比 25%,p<0.01)以及标准执行(95%比 80%,p=0.02)方面的表现更为优异。
该操作性方案通过生活方式风险识别、CHP 服务提供和标准执行来提高实施效果。在实施过程中应考虑未知的健康影响、偏倚和局限性,并进一步开展研究。
ClinicalTrials.gov:NCT01563575。注册日期:2012 年 3 月 27 日。https://clinicaltrials.gov/ct2/show/NCT01563575。