Nimmo Ailish M S A, McIntyre Sophie, Turner David M, Henderson Lorna K, Battle Richard K
Department of Renal Medicine, Royal Infirmary of Edinburgh, Edinburgh, United Kingdom.
Histocompatibility and Immunogenetics Laboratory, Scottish National Blood Transfusion Service, Royal Infirmary of Edinburgh, Edinburgh, United Kingdom.
Transplant Direct. 2018 Nov 23;4(12):e409. doi: 10.1097/TXD.0000000000000848. eCollection 2018 Dec.
The development of HLA antibodies towards a failing renal allograft is a barrier to retransplantation. This study aimed to compare the formation of HLA donor-specific antibodies (DSA) in patients undergoing graft nephrectomy and in those with a failed graft left in situ who had maintenance immunosuppression (IS) stopped, and assess the relative impact of IS cessation and graft nephrectomy on future relative chance of transplant (R-CoT).
A single-center retrospective study of patients with failed grafts between 2005 and 2015 was performed. Samples were tested for DSA pre-IS wean, post-IS wean, and post-IS cessation. Nephrectomy patients additionally had samples tested for DSA before and after nephrectomy. Calculated reaction frequency (cRF) was determined at each timepoint and entered into the UK Organ Donation and Transplant R-CoT calculator.
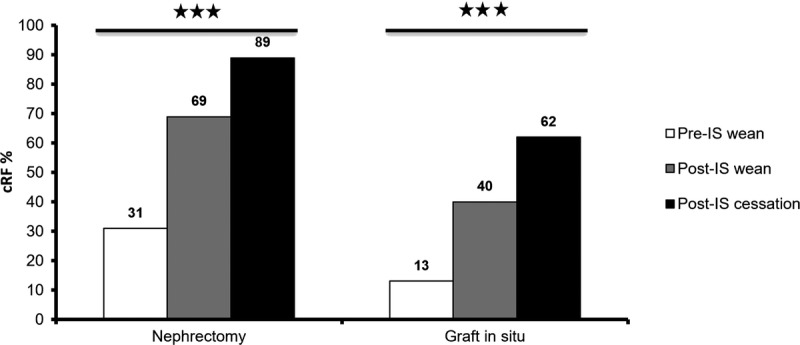
Forty-one patients were included in the study: 24 with nephrectomy and 17 with a failed graft in situ. Patient demographics and duration of IS wean were similar between groups. There was a higher rate of blood transfusion (54% vs 24%) in nephrectomy patients. In patients whose graft remained in situ, cRF rose from 13% pre-IS wean to 40% post-IS wean and 62% after IS cessation. This equated to a reduction in mean R-CoT from 54% to 46% at 5 years. In patients undergoing nephrectomy mean cRF rose from 31% pre-IS wean to 69% post-IS wean and 89% post-IS cessation. Mean R-CoT fell from 54% to 42% at 5 years.
A stepwise increase in cRF with reduced chance of transplant was observed in both groups as IS was withdrawn, with a similar pattern irrespective of graft nephrectomy. Calculated reaction frequency was higher in the nephrectomy group. The risks and benefits of stopping IS need to be carefully considered on an individual basis to maximize chance of future transplant.
针对失功肾移植受者产生的人类白细胞抗原(HLA)抗体是再次移植的障碍。本研究旨在比较接受移植肾切除术患者与移植肾失功但原位保留且停用维持性免疫抑制(IS)治疗患者中HLA供者特异性抗体(DSA)的形成情况,并评估停用IS和移植肾切除术对未来再次移植相对机会(R-CoT)的相对影响。
对2005年至2015年间移植肾失功患者进行单中心回顾性研究。在停用IS前、停用IS期间及停用IS后检测样本中的DSA。肾切除术患者在肾切除术前和术后额外检测DSA样本。在每个时间点确定计算反应频率(cRF),并将其输入英国器官捐赠和移植R-CoT计算器。
本研究共纳入41例患者:24例行肾切除术,17例移植肾原位失功。两组患者的人口统计学特征和停用IS的持续时间相似。肾切除术患者的输血率较高(54%对24%)。移植肾原位保留的患者,cRF从停用IS前的13%升至停用IS期间的40%,停用IS后为62%。这相当于5年时平均R-CoT从54%降至46%。接受肾切除术的患者,平均cRF从停用IS前的31%升至停用IS期间的69%,停用IS后为89%。5年时平均R-CoT从54%降至42%。
两组患者在停用IS时均观察到cRF逐步升高,移植机会降低,无论是否行移植肾切除术,模式相似。肾切除术组的计算反应频率更高。需要根据个体情况仔细考虑停用IS的风险和益处,以最大化未来移植的机会。