Institute for Exercise and Environmental Medicine, Texas Health Presbyterian Hospital Dallas and University of Texas Southwestern Medical Center, Dallas, TX.
Health Care Sciences, University of Texas Southwestern Medical Center, Dallas, TX.
Med Sci Sports Exerc. 2019 May;51(5):868-873. doi: 10.1249/MSS.0000000000001883.
The US Army's Standards of Medical Fitness, AR 40-501, state that "Prior burn injury (to include donor sites) involving a total body surface area of 40% or more does not meet the standard." Inclusion of donor sites (sites harvested for skin grafts) in this standard implies that thermoregulatory function is impaired within donor sites during exercise-heat stress; however, supporting evidence is currently lacking.
To test the hypothesis that well-healed donor and noninjured sites demonstrate similar elevations in skin blood flow and sweating during exercise-induced hyperthermia.
Twenty burn survivors (>1 yr postinjury; four females) cycled for 60 min in a 39.7°C ± 0.3°C and 21.1% ± 3.3% relative humidity environment at approximately 50% of maximal aerobic capacity. Core and mean skin temperatures were recorded throughout exercise. Skin blood flow (laser-Doppler imaging) was measured at baseline and after exercise within donor (LDFDON) and adjacent noninjured control (LDFCON) sites. At 45 min of exercise, local sweat rates (Technical Absorbents) were measured within the same donor (LSRDON) and noninjured (LSRCON) areas.
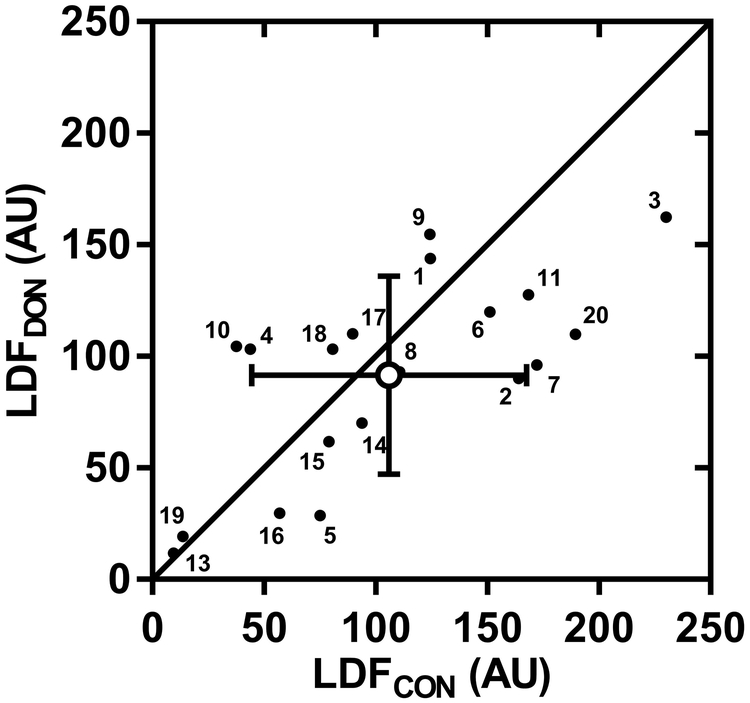
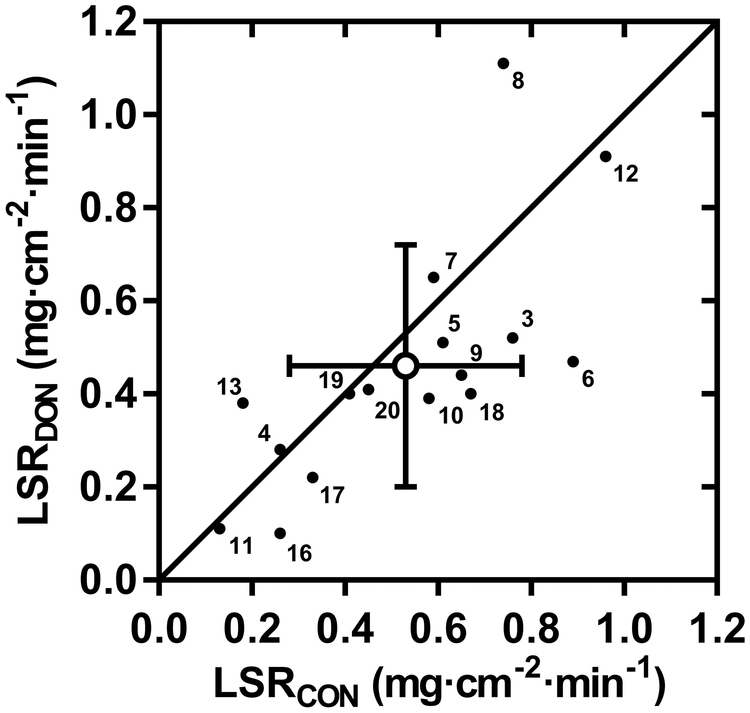
After 60 min of exercise, core and skin temperatures reached 38.2°C ± 0.4°C and 35.5°C ± 1.2°C, respectively. The increase in skin blood flow from baseline to end-exercise (LDFDON, 91.6 ± 44.5 AU; LDFCON, 106.0 ± 61.6 AU; P = 0.17) and local sweat rates (LSRDON, 0.46 ± 0.26 mg·cm·min; LSRCON, 0.53 ± 0.25 mg·cm·min; P = 0.14) were not different between donor and noninjured control sites.
Well-healed donor sites retain the ability to increase skin blood flow and sweating during exercise heat stress, providing evidence against the inclusion of donor sites when determining whether a burn injury meets the Army's Standards of Medical Fitness.
美国陆军医疗适应标准,AR 40-501,规定“先前的烧伤损伤(包括供体部位)总面积达到或超过 40%不符合标准。”在这个标准中包含供体部位(用于植皮的部位),这意味着在运动热应激期间,供体部位的体温调节功能受损;然而,目前缺乏支持证据。
测试以下假设,即愈合良好的供体部位和未受伤部位在运动引起的过热期间显示出相似的皮肤血流和出汗增加。
20 名烧伤幸存者(受伤后>1 年;4 名女性)在 39.7°C ± 0.3°C 和 21.1% ± 3.3%相对湿度的环境中以大约 50%最大有氧能力骑自行车 60 分钟。核心和平均皮肤温度在整个运动过程中都有记录。在运动前和运动后,使用激光多普勒成像(LDF)测量供体部位(LDFDON)和相邻未受伤对照部位(LDFCON)的皮肤血流。在运动 45 分钟时,在同一供体(LSRDON)和未受伤(LSRCON)区域内测量局部排汗率(技术吸收剂)。
运动 60 分钟后,核心和皮肤温度分别达到 38.2°C ± 0.4°C 和 35.5°C ± 1.2°C。从基线到运动结束时皮肤血流的增加(LDFDON,91.6 ± 44.5 AU;LDFCON,106.0 ± 61.6 AU;P = 0.17)和局部排汗率(LSRDON,0.46 ± 0.26 mg·cm·min;LSRCON,0.53 ± 0.25 mg·cm·min;P = 0.14)在供体和未受伤对照部位之间没有差异。
愈合良好的供体部位在运动热应激期间保留增加皮肤血流和出汗的能力,这一证据反对在确定烧伤损伤是否符合陆军医疗适应标准时包含供体部位。