Lund University, Lund, Sweden, and Broad Institute, Cambridge, Massachusetts.
Lund University, Lund, Sweden.
Arthritis Rheumatol. 2019 Jun;71(6):925-934. doi: 10.1002/art.40812. Epub 2019 Apr 17.
To investigate the causal role of cardiometabolic risk factors in osteoarthritis (OA) using associated genetic variants.
We studied 27,691 adults from the Malmö Diet and Cancer Study (MDCS) and replicated novel findings among 376,435 adults from the UK Biobank. Trait-specific polygenic risk scores for low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol levels, triglyceride levels, body mass index (BMI), fasting plasma glucose (FPG) levels, and systolic blood pressure (BP) were used to test the associations of genetically predicted elevations in each trait with incident OA diagnosis (n = 3,559), OA joint replacement (n = 2,780), or both (total OA; n = 4,226) in Mendelian randomization (MR) analyses in the MDCS, and with self-reported and/or hospital-diagnosed OA (n = 65,213) in the UK Biobank. Multivariable MR, MR-Egger, and weighted median MR were used to adjust for potential pleiotropic biases.
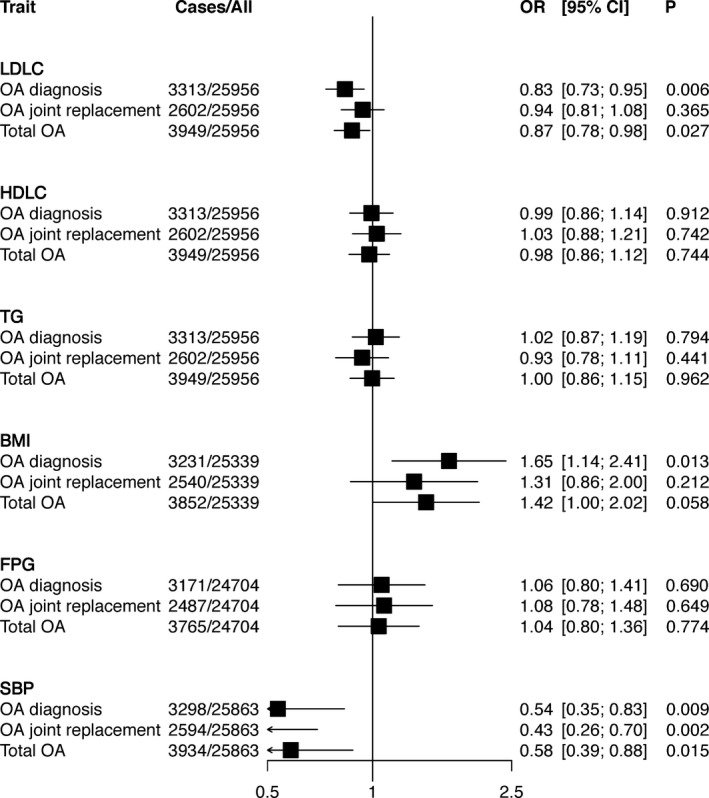
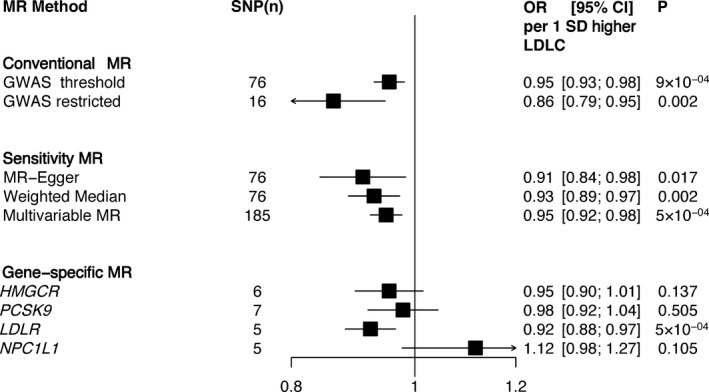
In the MDCS, genetically predicted elevation in LDL cholesterol level was associated with a lower risk of OA diagnosis (odds ratio [OR] 0.83 [95% confidence interval (95% CI) 0.73-0.95] per 1SD increase) and total OA (OR 0.87 [95% CI 0.78-0.98]), which was supported by multivariable MR for OA diagnosis (OR 0.84 [95% CI 0.75-0.95]) and total OA (0.87 [95% CI 0.78-0.97]), and by conventional 2-sample MR for OA diagnosis (OR 0.86 [95% CI 0.75-0.98]). MR-Egger indicated no pleiotropic bias. Genetically predicted elevation in BMI was associated with an increased risk of OA diagnosis (OR 1.65 [95% CI 1.14-2.41]), while MR-Egger indicated pleiotropic bias and a larger association with OA diagnosis (OR 3.25 [1.26-8.39]), OA joint replacement (OR 3.81 [95% CI 1.39-10.4]), and total OA (OR 3.41 [95% CI 1.43-8.15]). No associations were observed between genetically predicted HDL cholesterol level, triglyceride level, FPG level, or systolic BP and OA outcomes. The associations with LDL cholesterol levels were replicated in the UK Biobank (OR 0.95 [95% CI 0.93-0.98]).
Our MR study provides evidence of a causal role of lower LDL cholesterol level and higher BMI in OA.
利用相关的遗传变异来研究心血管代谢风险因素在骨关节炎(OA)中的因果作用。
我们研究了来自马尔默饮食与癌症研究(MDCS)的 27691 名成年人,并在来自英国生物库的 376435 名成年人中复制了新发现。使用特定于特质的载脂蛋白 LDL(LDL)和高密度脂蛋白(HDL)胆固醇水平、甘油三酯水平、体重指数(BMI)、空腹血糖(FPG)水平和收缩压(BP)的多基因风险评分来测试每种特质的遗传预测升高与新发 OA 诊断(n=3559)、OA 关节置换(n=2780)或两者(总 OA;n=4226)在 MDCS 中的孟德尔随机分析中的关联,以及在英国生物库中自我报告和/或医院诊断的 OA(n=65213)之间的关联。多变量 MR、MR-Egger 和加权中位数 MR 用于调整潜在的多效性偏倚。
在 MDCS 中,LDL 胆固醇水平升高的遗传预测与 OA 诊断风险降低相关(每增加 1SD,比值比[OR]为 0.83[95%置信区间(95%CI)为 0.73-0.95])和总 OA(OR 0.87[95%CI 为 0.78-0.98]),这得到了 OA 诊断多变量 MR(OR 0.84[95%CI 为 0.75-0.95])和总 OA(OR 0.87[95%CI 为 0.78-0.97])的支持,以及 OA 诊断常规 2 样本 MR(OR 0.86[95%CI 为 0.75-0.98])。MR-Egger 表明不存在多效性偏差。遗传预测 BMI 升高与 OA 诊断风险增加相关(OR 1.65[95%CI 为 1.14-2.41]),而 MR-Egger 表明存在多效性偏差和更大的关联与 OA 诊断(OR 3.25[1.26-8.39]),OA 关节置换(OR 3.81[95%CI 为 1.39-10.4])和总 OA(OR 3.41[95%CI 为 1.43-8.15])。遗传预测 HDL 胆固醇水平、甘油三酯水平、FPG 水平或收缩压与 OA 结果之间未观察到关联。在英国生物库中观察到 LDL 胆固醇水平与 OA 的关联(OR 0.95[95%CI 为 0.93-0.98])。
我们的 MR 研究提供了 LDL 胆固醇水平降低和 BMI 升高与 OA 之间存在因果关系的证据。