Mosepele Mosepele, Regan Susan, Massaro Joseph, Meigs James B, Zanni Markella V, D'Agostino Ralph B, Grinspoon Steven K, Triant Virginia A
Faculty of Medicine, University of Botswana.
Department of Immunology and Infectious Disease, Harvard School of Public Health, Boston, Massachusetts.
Open Forum Infect Dis. 2018 Dec 13;5(12):ofy326. doi: 10.1093/ofid/ofy326. eCollection 2018 Dec.
Individuals with human immunodeficiency virus (HIV) face elevated cardiovascular disease (CVD) risk. There are limited data regarding the application of the American College of Cardiology/American Heart Association (ACC/AHA) cholesterol guidelines in HIV compared with non-HIV patients.
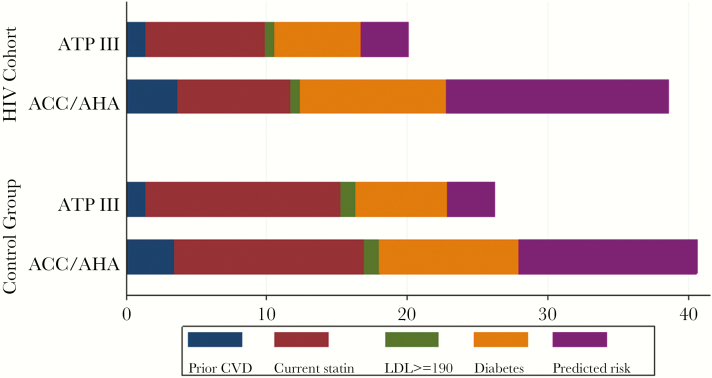
Human immunodeficiency virus-infected and demographically similar control patients were assessed for statin recommendation status by ACC/AHA and the National Cholesterol Education Program Adult Treatment Program III (ATPIII), indication for statin recommendation, actual statin prescription, and CVD event. Outcomes were atherosclerotic CVD for ACC/AHA and coronary heart disease for ATPIII.
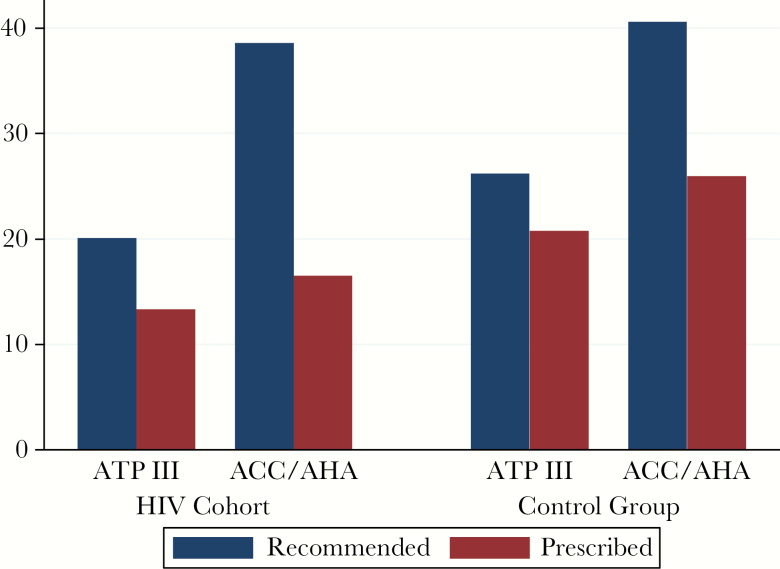
In a clinical care cohort of 1394 patients infected with HIV, 38.6% (538 of 1394) of patients were recommended for statin therapy by the ACC/AHA guidelines compared with 20.1% (280 of 1394) by the ATPIII guidelines. Of those recommended for statin therapy, actual statin prescription rates were 42.8% (230 of 538) for ACC/AHA and 66.4% (186 of 280) for ATPIII. Among patients infected with HIV with an incident CVD event during follow-up, statin therapy was recommended for 59.2% (42 of 71) of patients by ACC/AHA and 35.2% (25 of 71) by ATPIII, versus 71.6% (141 of 197) by ACC/AHA and 43.1% (85 of 197) by ATPIII in the control group.
In an HIV clinical care cohort, the ACC/AHA cholesterol guidelines recommend a higher proportion of patients for statin therapy and identify an increased proportion of patients with a CVD event compared with ATPIII. However, 40% of patients with a CVD event would not have been recommended for statin therapy by ACC/AHA, compared with 29% for controls. This gap in identification of patients infected with HIV at high CVD risk underscores the need for HIV-specific cardiovascular prevention strategies.
感染人类免疫缺陷病毒(HIV)的个体面临更高的心血管疾病(CVD)风险。与未感染HIV的患者相比,关于美国心脏病学会/美国心脏协会(ACC/AHA)胆固醇指南在HIV患者中的应用数据有限。
对感染HIV的患者及人口统计学特征相似的对照患者进行评估,以确定ACC/AHA和国家胆固醇教育计划成人治疗计划III(ATPIII)的他汀类药物推荐状态、他汀类药物推荐的指征、实际他汀类药物处方情况以及CVD事件。ACC/AHA的结局指标为动脉粥样硬化性CVD,ATPIII的结局指标为冠心病。
在一个包含1394例HIV感染患者的临床护理队列中,ACC/AHA指南推荐38.6%(1394例中的538例)的患者接受他汀类药物治疗,而ATPIII指南推荐20.1%(1394例中的280例)。在那些被推荐接受他汀类药物治疗的患者中,ACC/AHA的实际他汀类药物处方率为42.8%(538例中的230例),ATPIII为66.4%(280例中的186例)。在随访期间发生CVD事件的HIV感染患者中,ACC/AHA推荐59.2%(71例中的42例)的患者接受他汀类药物治疗,ATPIII推荐35.2%(71例中的25例);而在对照组中,ACC/AHA推荐71.6%(197例中的141例),ATPIII推荐43.1%(197例中的85例)。
在一个HIV临床护理队列中,与ATPIII相比,ACC/AHA胆固醇指南推荐接受他汀类药物治疗的患者比例更高,且识别出的CVD事件患者比例增加。然而,ACC/AHA不会推荐40%发生CVD事件的HIV感染患者接受他汀类药物治疗,而对照组这一比例为29%。在识别高CVD风险的HIV感染患者方面存在的这一差距凸显了制定针对HIV的心血管预防策略的必要性。