Division of General Internal Medicine (V.A.T, S.R., J.B.M.)
Division of Infectious Diseases (V.A.T.).
Circulation. 2018 May 22;137(21):2203-2214. doi: 10.1161/CIRCULATIONAHA.117.028975. Epub 2018 Feb 14.
Cardiovascular disease (CVD) risk is elevated in HIV-infected individuals, with contributions from both traditional and nontraditional risk factors. The accuracy of established CVD risk prediction functions in HIV is uncertain. We sought to assess the performance of 3 established CVD risk prediction functions in a longitudinal cohort of HIV-infected men.
The FHS (Framingham Heart Study) functions for hard coronary heart disease (FHS CHD) and atherosclerotic CVD (FHS ASCVD) and the American College of Cardiology/American Heart Association ASCVD function were applied to the Partners HIV cohort. Risk scores were calculated between January 1, 2006, and December 31, 2008. Outcomes included CHD (myocardial infarction or coronary death) for the FHS CHD function and ASCVD (myocardial infarction, stroke, or coronary death) for the FHS ASCVD and American College of Cardiology/American Heart Association ASCVD functions. We investigated the accuracy of CVD risk prediction for each function when applied to the HIV cohort using comparison of Cox regression coefficients, discrimination, and calibration.
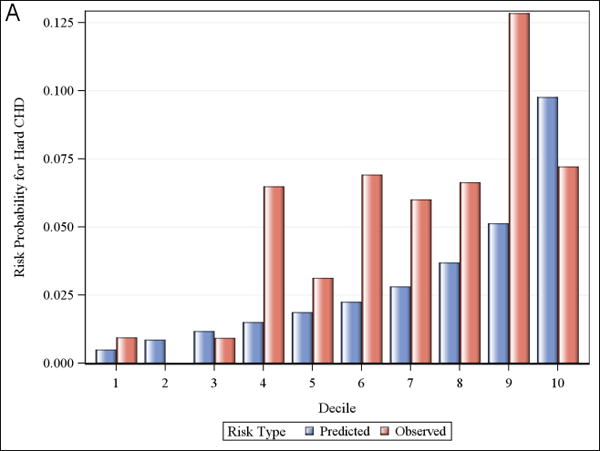
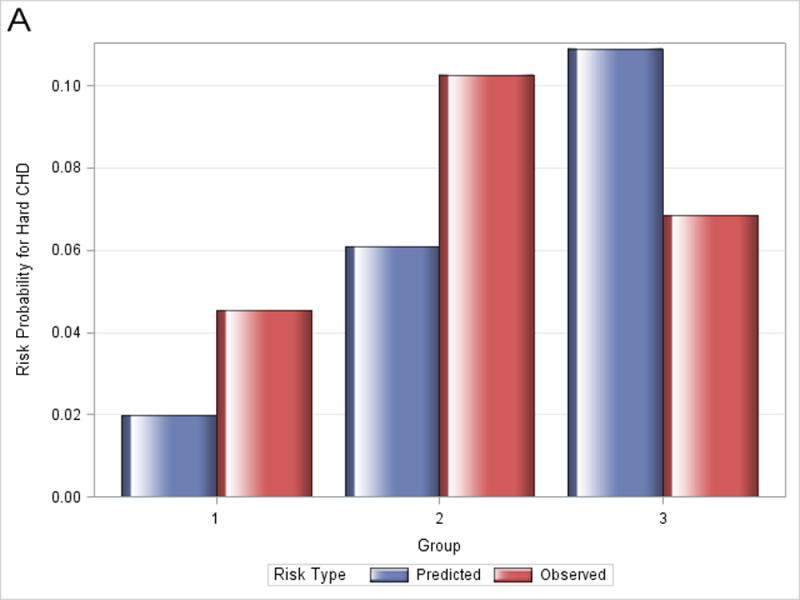
The HIV cohort was comprised of 1272 men followed for a median of 4.4 years. There were 78 (6.1%) ASCVD events; the 5-year incidence rate was 16.4 per 1000 person-years. Discrimination was moderate to poor as indicated by the low statistic (0.68 for FHS CHD, 0.65 for American College of Cardiology/American Heart Association ASCVD, and 0.67 for FHS ASCVD). Observed CVD risk exceeded the predicted risk for each of the functions in most deciles of predicted risk. Calibration, or goodness of fit of the models, was consistently poor, with significant χ values for all functions. Recalibration did not significantly improve model fit.
Cardiovascular risk prediction functions developed for use in the general population are inaccurate in HIV infection and systematically underestimate risk in a cohort of HIV-infected men. Development of tailored CVD risk prediction functions incorporating traditional CVD risk factors and HIV-specific factors is likely to result in more accurate risk estimation to guide preventative CVD care.
心血管疾病 (CVD) 风险在感染 HIV 的个体中升高,其原因既有传统风险因素,也有非传统风险因素。在 HIV 中,既定 CVD 风险预测函数的准确性尚不确定。我们旨在评估 3 种既定 CVD 风险预测函数在 HIV 感染男性纵向队列中的表现。
Framingham 心脏研究 (FHS) 的硬冠状动脉心脏病 (FHS CHD) 和动脉粥样硬化性 CVD (FHS ASCVD) 功能以及美国心脏病学会/美国心脏协会 ASCVD 功能应用于 Partners HIV 队列。风险评分在 2006 年 1 月 1 日至 2008 年 12 月 31 日之间计算。结局包括 FHS CHD 功能的 CHD(心肌梗死或冠状动脉死亡)和 FHS ASCVD 和美国心脏病学会/美国心脏协会 ASCVD 功能的 ASCVD(心肌梗死、卒中和冠状动脉死亡)。我们通过比较 Cox 回归系数、区分度和校准来研究每种功能应用于 HIV 队列时 CVD 风险预测的准确性。
HIV 队列由 1272 名男性组成,中位随访时间为 4.4 年。有 78 例(6.1%)ASCVD 事件;5 年发生率为每 1000 人年 16.4 例。区分度为中度至较差,低统计量表明(FHS CHD 为 0.68,美国心脏病学会/美国心脏协会 ASCVD 为 0.65,FHS ASCVD 为 0.67)。在预测风险的大多数十分位数中,观察到的 CVD 风险超过了每个功能的预测风险。模型的校准或拟合度均较差,所有功能的 χ 值均有显著差异。重新校准并未显著改善模型拟合度。
为一般人群开发的心血管风险预测函数在 HIV 感染中不准确,并且系统地低估了 HIV 感染男性队列的风险。开发纳入传统 CVD 风险因素和 HIV 特异性因素的定制 CVD 风险预测函数可能会导致更准确的风险估计,以指导预防性 CVD 护理。