Toribio Mabel, Fitch Kathleen V, Sanchez Laura, Burdo Tricia H, Williams Kenneth C, Sponseller Craig A, McCurdy Pate Mary, Aberg Judith A, Zanni Markella V, Grinspoon Steven K
aMassachusetts General Hospital, Program in Nutrition and Metabolism and Harvard Medical School, Boston bDepartment of Biology, Boston College, Chestnut Hill, Massachusetts cDepartment of Neuroscience, Temple University School of Medicine, Philadelphia, Pennsylvania dMount Sinai Department of Medicine, Division of Infectious Diseases, Icahn School of Medicine at Mount Sinai, New York, New York eKOWA Pharmaceuticals America Inc., Montgomery, Alabama, USA.
AIDS. 2017 Mar 27;31(6):797-806. doi: 10.1097/QAD.0000000000001427.
Persistent immune activation is thought to contribute to increased cardiovascular disease risk in HIV and statins may help modulate systemic immune activation. We aimed to compare the effects of two key statins on markers of systemic immune activation and arterial inflammation in the HIV population.
Double-blind, active-controlled, parallel-group comparative trial performed in 45 sites.
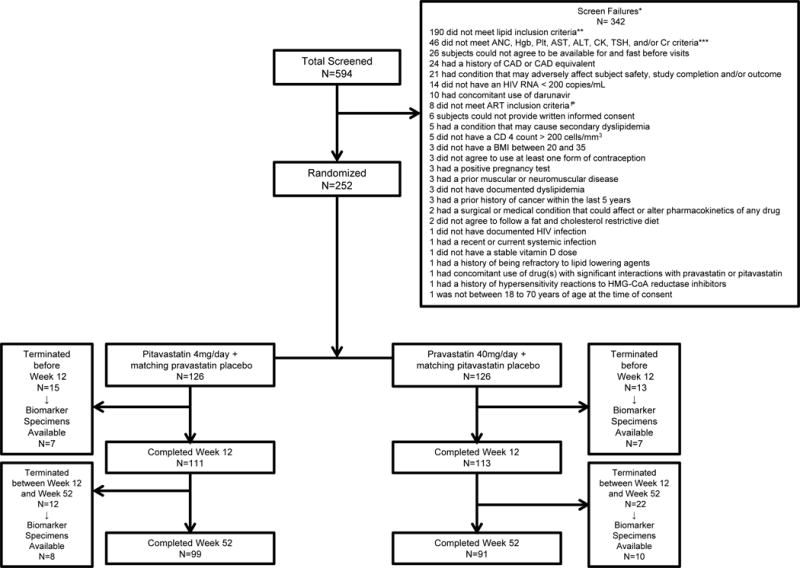
Two hundred and fifty-two antiretroviral therapy-treated HIV-infected participants with dyslipidemia were randomized (1 : 1) to pitavastatin 4 mg daily vs. pravastatin 40 mg daily in the HIV-infected patieNts and TREatment with PItavastatin vs. pravastatin for Dyslipidemia (INTREPID) trial. In this analysis of the INTREPID trial, we assessed markers of immune activation and arterial inflammation using a modified intent-to-treat population. This trial is registered with ClinicalTrials.gov (NCT01301066).
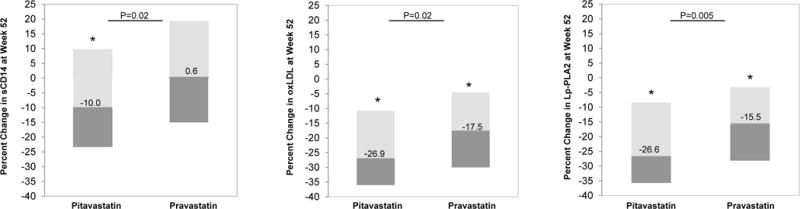
One hundred and twenty-six participants were randomized to receive pitavastatin and 126 to pravastatin. Ninety-nine participants in the pitavastatin group and 91 participants in the pravastatin group completed the study. Median age was 50 (45, 56) years [median (interquartile range)]. Baseline, low-density lipoprotein-cholestrol (LDL-C) was 153 (135, 171) mg/dl, log HIV-1 viral load was 1.1 ± 0.2 copies/ml, and CD4 cell count was 580 (439, 794) cells/μl. At week 52, the pitavastatin group had a significantly greater reduction (% change) compared with pravastatin in soluble CD14 (sCD14), (-10.0 vs. 0.6%, P = 0.02), oxidized LDL (oxLDL) (-26.9 vs. -17.5%, P = 0.02), and lipoprotein-associated phospholipase 2 (Lp-PLA2) (-26.6 vs. -15.5%, P = 0.005) (pitavastatin vs. pravastatin).
Fifty-two weeks of pitavastatin 4 mg daily (vs. pravastatin 40 mg daily) led to a greater reduction in select markers of immune activation and arterial inflammation (sCD14, oxLDL, and LpPLA2) among HIV-infected participants. Further work is needed to assess whether immune-modulatory effects of pitavastatin reduce cardiovascular disease risk in HIV.
持续性免疫激活被认为会增加HIV感染者患心血管疾病的风险,而他汀类药物可能有助于调节全身免疫激活。我们旨在比较两种关键他汀类药物对HIV感染者全身免疫激活标志物和动脉炎症的影响。
在45个地点进行的双盲、活性对照、平行组比较试验。
252名接受抗逆转录病毒治疗且患有血脂异常的HIV感染者被随机(1:1)分为两组,一组每天服用4毫克匹伐他汀,另一组每天服用40毫克普伐他汀,该试验为HIV感染者匹伐他汀与普伐他汀治疗血脂异常(INTREPID)试验。在对INTREPID试验的此次分析中,我们使用改良的意向性治疗人群评估免疫激活和动脉炎症标志物。该试验已在ClinicalTrials.gov注册(NCT01301066)。
126名参与者被随机分配接受匹伐他汀治疗,126名接受普伐他汀治疗。匹伐他汀组99名参与者和普伐他汀组91名参与者完成了研究。中位年龄为50(45,56)岁[中位数(四分位间距)]。基线时,低密度脂蛋白胆固醇(LDL-C)为153(135,171)mg/dl,HIV-1病毒载量对数为1.1±0.2拷贝/ml,CD4细胞计数为580(439,794)个/μl。在第52周时,与普伐他汀相比,匹伐他汀组可溶性CD14(sCD14)的降低幅度(%变化)显著更大(-10.0%对0.6%,P = 0.02)、氧化型低密度脂蛋白(oxLDL)(-26.9%对-17.5%,P = 0.02)以及脂蛋白相关磷脂酶2(Lp-PLA2)(-26.6%对-15.5%,P = 0.005)(匹伐他汀组对普伐他汀组)。
在HIV感染者中,每天服用4毫克匹伐他汀(对比每天服用40毫克普伐他汀)持续52周可使免疫激活和动脉炎症的特定标志物(sCD14、oxLDL和LpPLA2)有更大幅度的降低。需要进一步开展工作来评估匹伐他汀的免疫调节作用是否能降低HIV感染者患心血管疾病的风险。