Burden of Disease Epidemiology, Equity and Cost-Effectiveness Programme, Department of Public Health, University of Otago, Wellington, New Zealand.
Melbourne School of Population and Global Health, University of Melbourne, Melbourne, Australia.
PLoS Med. 2019 Jan 8;16(1):e1002716. doi: 10.1371/journal.pmed.1002716. eCollection 2019 Jan.
There is little systematic assessment of how total health expenditure is distributed across diseases and comorbidities. The objective of this study was to use statistical methods to disaggregate all publicly funded health expenditure by disease and comorbidities in order to answer three research questions: (1) What is health expenditure by disease phase for noncommunicable diseases (NCDs) in New Zealand? (2) Is the cost of having two NCDs more or less than that expected given the independent costs of each NCD? (3) How is total health spending disaggregated by NCDs across age and by sex?
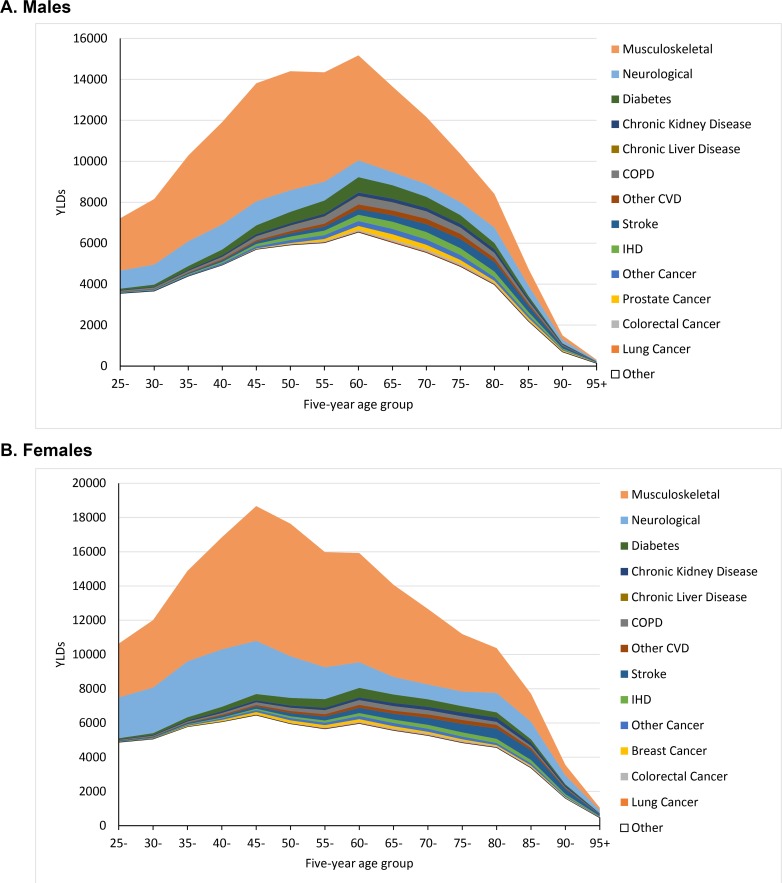
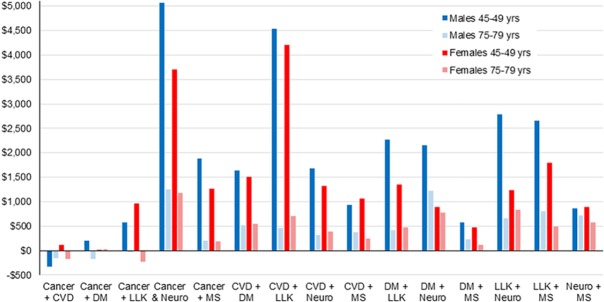
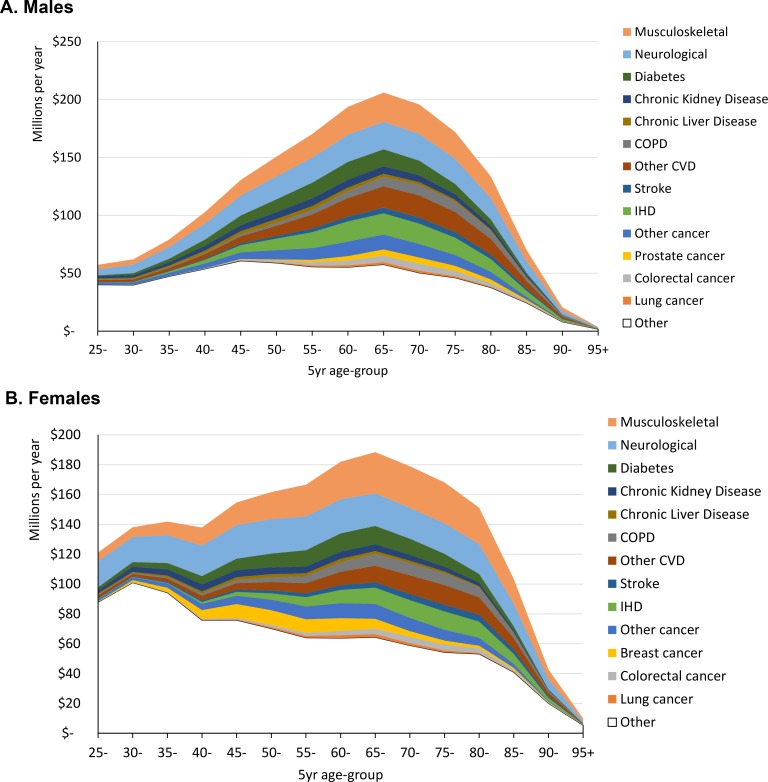
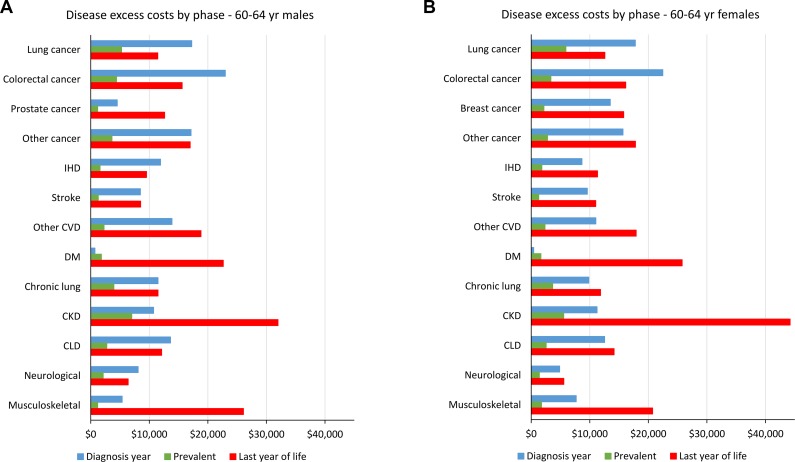
We used linked data for all adult New Zealanders for publicly funded events, including hospitalisation, outpatient, pharmaceutical, laboratory testing, and primary care from 1 July 2007 to 30 June 2014. These data include 18.9 million person-years and $26.4 billion in spending (US$ 2016). We used case definition algorithms to identify if a person had any of six NCDs (cancer, cardiovascular disease [CVD], diabetes, musculoskeletal, neurological, and a chronic lung/liver/kidney [LLK] disease). Indicator variables were used to identify the presence of any of the 15 possible comorbidity pairings of these six NCDs. Regression was used to estimate excess annual health expenditure per person. Cause deletion methods were used to estimate total population expenditure by disease. A majority (59%) of health expenditure was attributable to NCDs. Expenditure due to diseases was generally highest in the year of diagnosis and year of death. A person having two diseases simultaneously generally had greater health expenditure than the expected sum of having the diseases separately, for all 15 comorbidity pairs except the CVD-cancer pair. For example, a 60-64-year-old female with none of the six NCDs had $633 per annum expenditure. If she had both CVD and chronic LLK, additional expenditure for CVD separately was $6,443/$839/$9,225 for the first year of diagnosis/prevalent years/last year of life if dying of CVD; additional expenditure for chronic LLK separately was $6,443/$1,291/$9,051; and the additional comorbidity expenditure of having both CVD and LLK was $2,456 (95% confidence interval [CI] $2,238-$2,674). The pattern was similar for males (e.g., additional comorbidity expenditure for a 60-64-year-old male with CVD and chronic LLK was $2,498 [95% CI $2,264-$2,632]). In addition to this, the excess comorbidity costs for a person with two diseases was greater at younger ages, e.g., excess expenditure for 45-49-year-old males with CVD and chronic LLK was 10 times higher than for 75-79-year-old males and six times higher for females. At the population level, 23.8% of total health expenditure was attributable to higher costs of having one of the 15 comorbidity pairs over and above the six NCDs separately; of the remaining expenditure, CVD accounted for 18.7%, followed by musculoskeletal (16.2%), neurological (14.4%), cancer (14.1%), chronic LLK disease (7.4%), and diabetes (5.5%). Major limitations included incomplete linkage to all costed events (although these were largely non-NCD events) and missing private expenditure.
The costs of having two NCDs simultaneously is typically superadditive, and more so for younger adults. Neurological and musculoskeletal diseases contributed the largest health system costs, in accord with burden of disease studies finding that they contribute large morbidity. Just as burden of disease methodology has advanced the understanding of disease burden, there is a need to create disease-based costing studies that facilitate the disaggregation of health budgets at a national level.
目前对于总医疗支出在疾病和合并症之间的分布情况,尚未有系统的评估。本研究旨在运用统计学方法,对所有由公共资金支付的疾病和合并症进行细分,以回答三个研究问题:(1)新西兰的非传染性疾病(NCD)各阶段的健康支出是多少?(2)同时患有两种 NCD 的成本是否高于每种 NCD 各自的预期成本?(3)按疾病和年龄及性别对总医疗支出进行细分的情况如何?
我们使用了 2007 年 7 月 1 日至 2014 年 6 月 30 日期间,所有新西兰成年人的公共资金支付的事件相关数据,包括住院、门诊、药物、实验室检查和初级保健。这些数据包括 1890 万人年和 264 亿美元(2016 年美元)的支出。我们使用病例定义算法来确定一个人是否患有六种 NCD 中的任何一种(癌症、心血管疾病[CVD]、糖尿病、肌肉骨骼、神经和慢性肺/肝/肾[LLK]疾病)。使用指示变量来确定是否存在这六种 NCD 中任何 15 种可能的合并症配对。回归用于估计每个人每年的超额健康支出。因果删除方法用于按疾病估计总人口支出。大多数(59%)的健康支出归因于 NCD。疾病支出通常在诊断年和死亡年最高。对于所有 15 种合并症配对,患有两种疾病的人通常比单独患有这两种疾病的人有更高的健康支出,除了 CVD-癌症配对。例如,一个 60-64 岁的女性没有任何六种 NCD,她每年的支出为 633 美元。如果她同时患有 CVD 和慢性 LLK,如果 CVD 是诊断年/流行年/死亡年,那么单独患有 CVD 的额外支出分别为 6443 美元/1291 美元/9051 美元;单独患有慢性 LLK 的额外支出分别为 6443 美元/1291 美元/9051 美元;同时患有 CVD 和 LLK 的合并症支出为 2456 美元(95%置信区间[CI]2238-2674 美元)。对于男性来说,情况类似(例如,一位 60-64 岁患有 CVD 和慢性 LLK 的男性的额外合并症支出为 2498 美元[95%CI2264-2632 美元])。除此之外,患有两种疾病的人的合并症成本在较年轻时更高,例如,45-49 岁男性的 CVD 和慢性 LLK 合并症支出是 75-79 岁男性的 10 倍,女性的 6 倍。在人群层面上,总健康支出的 23.8%归因于超过六种 NCD 分别单独的成本的 15 种合并症配对之一的更高成本;其余支出中,CVD 占 18.7%,其次是肌肉骨骼(16.2%)、神经(14.4%)、癌症(14.1%)、慢性 LLK 疾病(7.4%)和糖尿病(5.5%)。主要限制包括不完全链接到所有计费事件(尽管这些主要是非 NCD 事件)和缺失的私人支出。
同时患有两种 NCD 的成本通常是超相加的,对于年轻成年人来说更是如此。神经和肌肉骨骼疾病导致了最大的医疗系统成本,这与疾病负担研究发现它们导致了大量的发病率相符。正如疾病负担方法学已经提高了对疾病负担的理解一样,需要创建基于疾病的成本研究,以便在国家层面上对卫生预算进行细分。