Khalil Asma, Duffy James M N, Perry Helen, Ganzevoort Wessel, Reed Keith, Baschat Ahmet A, Deprest Jan, Gratacos Eduardo, Hecher Kurt, Lewi Liesbeth, Lopriore Enrico, Oepkes Dick, Papageorghiou Aris, Gordijn Sanne J
Vascular Biology Research Centre, Molecular and Clinical Sciences Research Institute, St George's University of London, Cranmer Terrace, London, SW17 0RE, UK.
Fetal Medicine Unit, Department of Obstetrics and Gynaecology, St. George's University Hospitals NHS Foundation Trust, Blackshaw Road, London, SW17 0QT, UK.
Trials. 2019 Jan 9;20(1):35. doi: 10.1186/s13063-018-3153-y.
Selective fetal growth restriction in monochorionic twin pregnancies is associated with an increased risk of perinatal mortality and morbidity and represents a clinical dilemma. Interventions include expectant management with early preterm delivery if there are signs of fetal compromise, selective termination of the compromised twin, fetoscopic laser coagulation of the communicating placental vessels or termination of the whole pregnancy. Previous studies evaluating interventions have reported many different outcomes and outcome measures. Such variation makes comparing, contrasting, and combining results challenging, limiting ongoing research on this uncommon condition to inform clinical practice. We aim to produce, disseminate, and implement a core outcome set for selective fetal growth restriction research in monochorionic twin pregnancies.
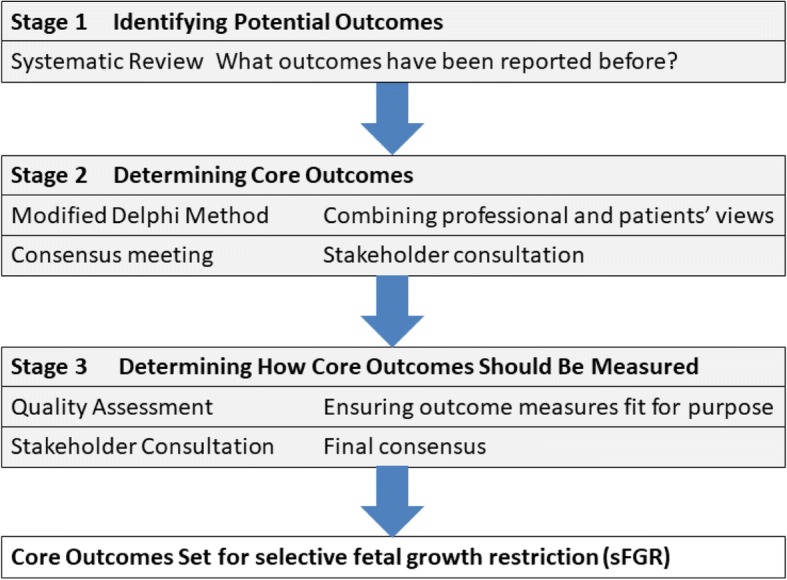
An international steering group, including professionals, researchers, and lay experts, has been established to oversee the development of this core outcome set. The methods have been guided by the Core Outcome Measures in Effectiveness Trials Initiative Handbook. Potential core outcomes will be developed by undertaking a systematic review of studies evaluating interventions for selective fetal growth restriction in monochorionic twin pregnancies. Potential core outcomes will be entered into a three-round Delphi survey and key stakeholders including clinical professionals, researchers, and lay experts will be invited to participate. Repeated reflection and rescoring of individual outcomes should encourage group and individual stakeholder convergence towards consensus outcomes which will be entered into a modified Nominal Group Technique to finalize the core outcome set. Once core outcomes have been agreed, we will establish standardized definitions and recommend high-quality measurement instruments for each outcome.
The development, dissemination, and implementation of a core outcome set for selective fetal growth restriction should ensure that future research protocols select, collect, and report outcomes and outcome measures in a standardized manner. Data synthesis will be possible on a broad level and rigorous implementation should advance the quality of research studies and their effective use in order to guide clinical practice, improve patient care, maternal, short-term perinatal outcomes, and long-term neurodevelopmental outcomes.
Core Outcome Measures in Effectiveness Trials (COMET) registration number: 998. International Prospective Register of Systematic Reviews (PROSPERO) registration number: CRD42018092697 . 18th April 2018.
单绒毛膜双胎妊娠中的选择性胎儿生长受限与围产期死亡率和发病率增加相关,是一个临床难题。干预措施包括若有胎儿窘迫迹象则进行期待治疗并尽早早产、选择性终止受影响的胎儿、胎儿镜下激光凝固胎盘交通血管或终止整个妊娠。以往评估干预措施的研究报告了许多不同的结果和结局指标。这种差异使得比较、对比和整合结果具有挑战性,限制了针对这种罕见情况的正在进行的研究为临床实践提供信息。我们旨在制定、传播和实施一个单绒毛膜双胎妊娠选择性胎儿生长受限研究的核心结局集。
已成立一个国际指导小组,包括专业人员、研究人员和非专业专家,以监督该核心结局集的制定。方法遵循有效性试验核心结局指标倡议手册。潜在的核心结局将通过对评估单绒毛膜双胎妊娠选择性胎儿生长受限干预措施的研究进行系统评价来确定。潜在的核心结局将纳入三轮德尔菲调查,并邀请包括临床专业人员、研究人员和非专业专家在内的关键利益相关者参与。对个体结局进行反复思考和重新评分应促使团体和个体利益相关者趋向于达成共识结局,这些结局将纳入改良的名义小组技术以最终确定核心结局集。一旦核心结局达成一致,我们将为每个结局建立标准化定义并推荐高质量的测量工具。
选择性胎儿生长受限核心结局集的制定、传播和实施应确保未来的研究方案以标准化方式选择、收集和报告结局及结局指标。在广泛层面上进行数据综合将成为可能,严格实施应提高研究的质量及其有效利用,以指导临床实践、改善患者护理、孕产妇、短期围产期结局和长期神经发育结局。
有效性试验核心结局指标(COMET)注册号:998。国际系统评价前瞻性注册库(PROSPERO)注册号:CRD42018092697。2018年4月18日。