Kidney Health Research Institute, and Department of Epidemiology and Health Services Research, Geisinger Health System, Danville, PA, USA.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
BMJ. 2019 Jan 10;364:k5301. doi: 10.1136/bmj.k5301.
To evaluate the associations between adiposity measures (body mass index, waist circumference, and waist-to-height ratio) with decline in glomerular filtration rate (GFR) and with all cause mortality.
Individual participant data meta-analysis.
Cohorts from 40 countries with data collected between 1970 and 2017.
Adults in 39 general population cohorts (n=5 459 014), of which 21 (n=594 496) had data on waist circumference; six cohorts with high cardiovascular risk (n=84 417); and 18 cohorts with chronic kidney disease (n=91 607).
GFR decline (estimated GFR decline ≥40%, initiation of kidney replacement therapy or estimated GFR <10 mL/min/1.73 m) and all cause mortality.
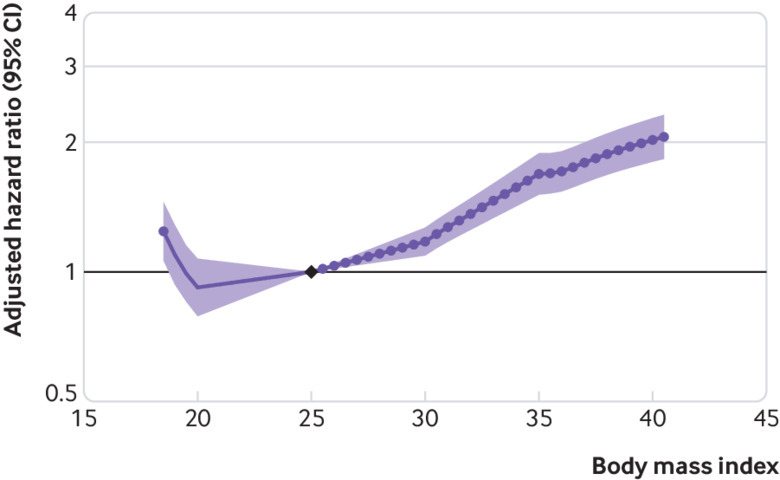
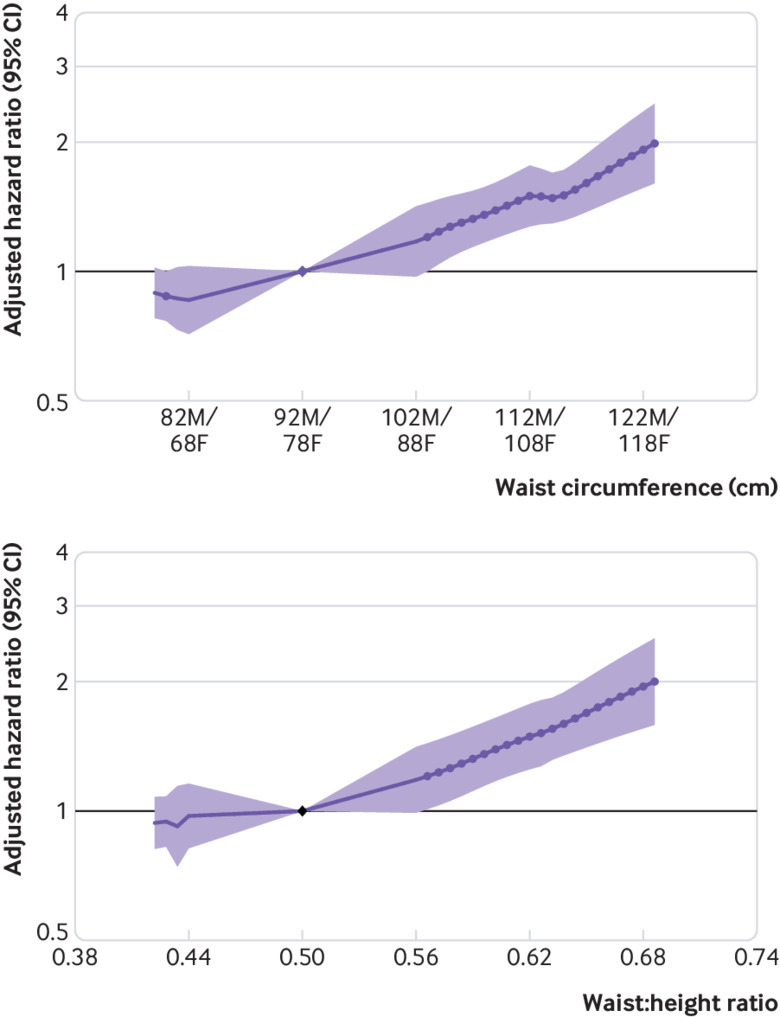
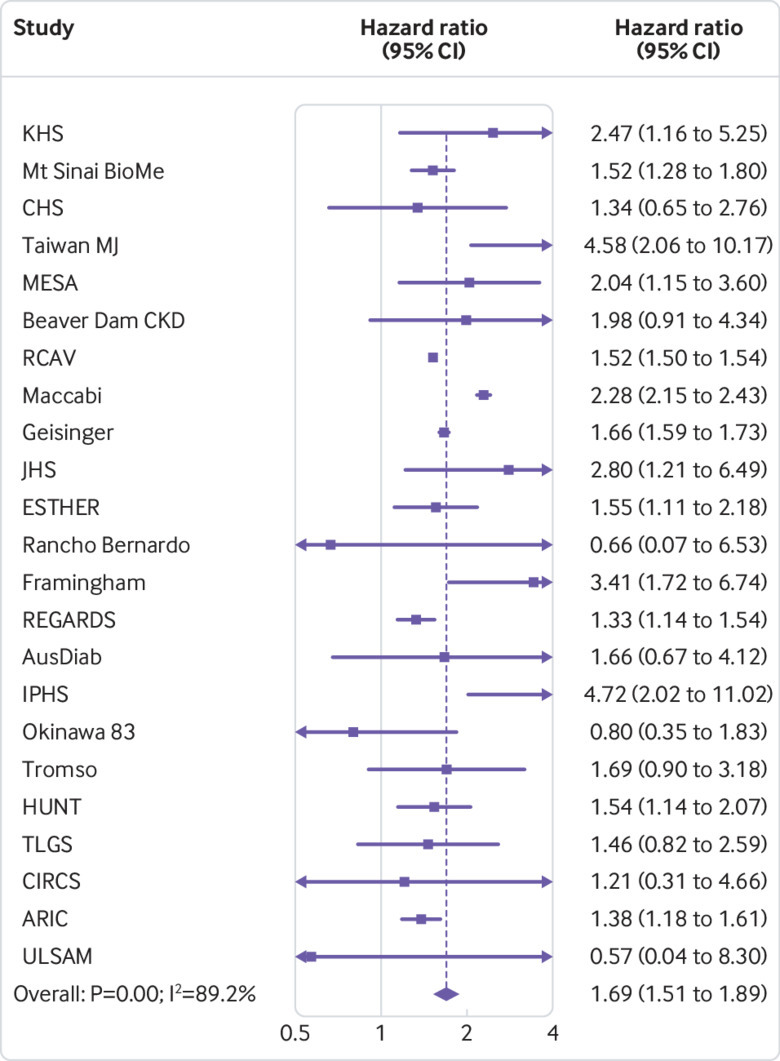
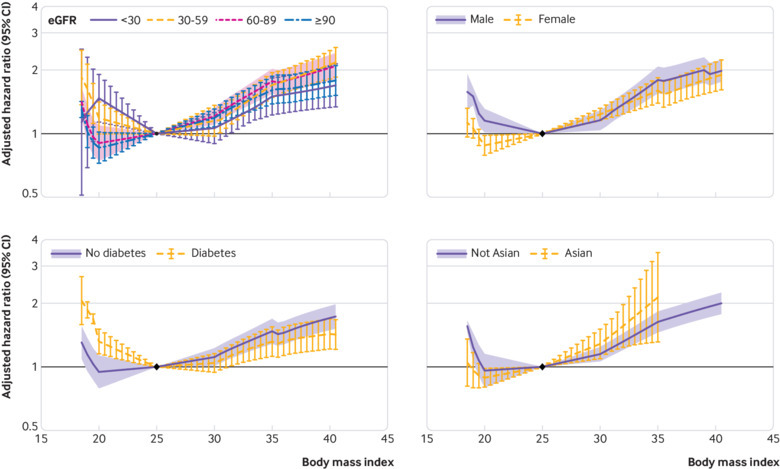
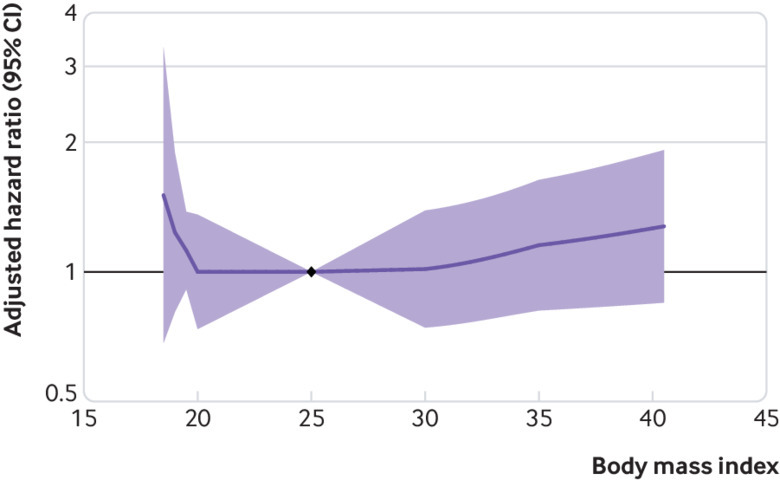
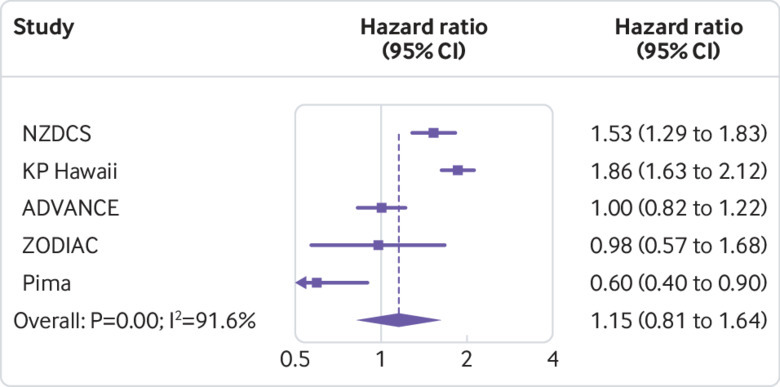
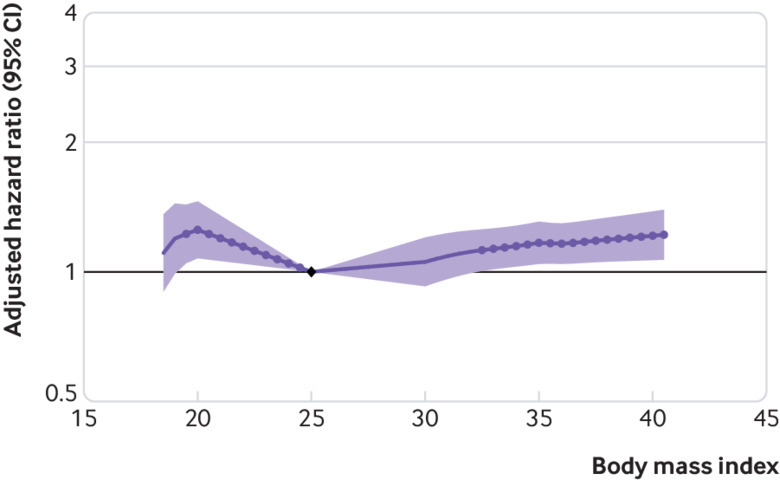
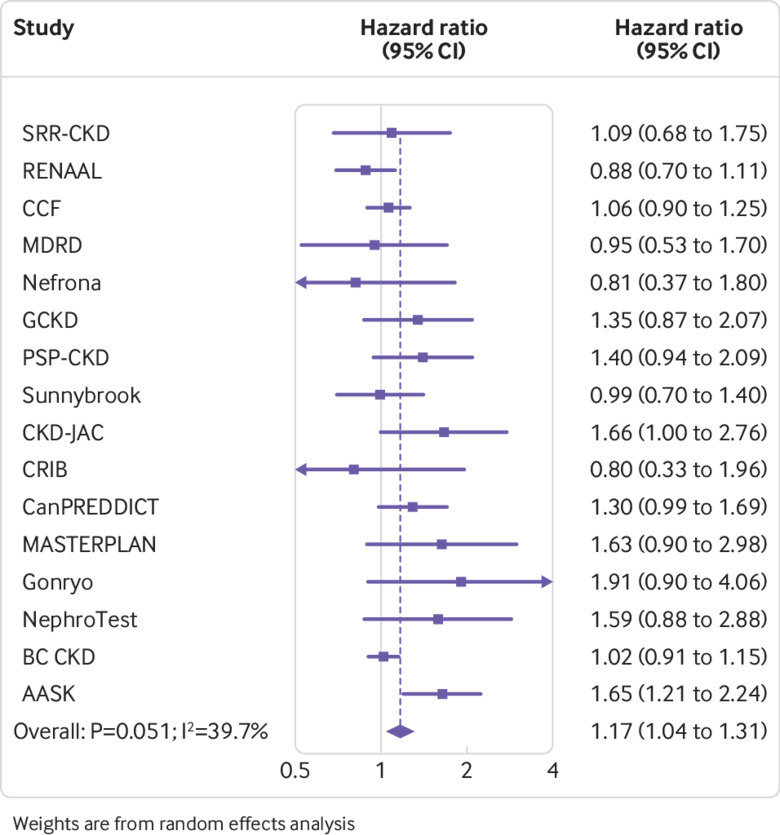
Over a mean follow-up of eight years, 246 607 (5.6%) individuals in the general population cohorts had GFR decline (18 118 (0.4%) end stage kidney disease events) and 782 329 (14.7%) died. Adjusting for age, sex, race, and current smoking, the hazard ratios for GFR decline comparing body mass indices 30, 35, and 40 with body mass index 25 were 1.18 (95% confidence interval 1.09 to 1.27), 1.69 (1.51 to 1.89), and 2.02 (1.80 to 2.27), respectively. Results were similar in all subgroups of estimated GFR. Associations weakened after adjustment for additional comorbidities, with respective hazard ratios of 1.03 (0.95 to 1.11), 1.28 (1.14 to 1.44), and 1.46 (1.28 to 1.67). The association between body mass index and death was J shaped, with the lowest risk at body mass index of 25. In the cohorts with high cardiovascular risk and chronic kidney disease (mean follow-up of six and four years, respectively), risk associations between higher body mass index and GFR decline were weaker than in the general population, and the association between body mass index and death was also J shaped, with the lowest risk between body mass index 25 and 30. In all cohort types, associations between higher waist circumference and higher waist-to-height ratio with GFR decline were similar to that of body mass index; however, increased risk of death was not associated with lower waist circumference or waist-to-height ratio, as was seen with body mass index.
Elevated body mass index, waist circumference, and waist-to-height ratio are independent risk factors for GFR decline and death in individuals who have normal or reduced levels of estimated GFR.
评估肥胖指标(体重指数、腰围和腰高比)与肾小球滤过率(GFR)下降和全因死亡率之间的关联。
个体参与者数据荟萃分析。
1970 年至 2017 年间来自 40 个国家的队列数据。
来自 39 个一般人群队列的成年人(n=5459014),其中 21 个队列(n=594496)有腰围数据;6 个心血管风险较高的队列(n=84417);18 个慢性肾脏病队列(n=91607)。
GFR 下降(估计 GFR 下降≥40%,开始肾脏替代治疗或估计 GFR<10 mL/min/1.73 m)和全因死亡率。
在平均 8 年的随访中,一般人群队列中有 246607 人(5.6%)出现 GFR 下降(18118 人(0.4%)发生终末期肾病事件),782329 人(14.7%)死亡。在调整年龄、性别、种族和当前吸烟状况后,与体重指数 25 相比,体重指数 30、35 和 40 的 GFR 下降的风险比分别为 1.18(95%置信区间 1.09 至 1.27)、1.69(1.51 至 1.89)和 2.02(1.80 至 2.27)。在估计 GFR 的所有亚组中,结果均相似。在调整其他合并症后,关联减弱,相应的风险比分别为 1.03(0.95 至 1.11)、1.28(1.14 至 1.44)和 1.46(1.28 至 1.67)。体重指数与死亡的关联呈 J 型,体重指数为 25 时风险最低。在心血管风险较高和慢性肾脏病队列(分别为平均随访 6 年和 4 年)中,较高体重指数与 GFR 下降之间的风险关联弱于一般人群,体重指数与死亡之间的关联也呈 J 型,体重指数在 25 至 30 之间时风险最低。在所有队列类型中,较高腰围和腰高比与 GFR 下降的关联与体重指数相似;然而,较低的腰围或腰高比与死亡率的增加无关,这与体重指数的情况相同。
在肾小球滤过率正常或降低的个体中,升高的体重指数、腰围和腰高比是 GFR 下降和死亡的独立危险因素。