Morris Mackenzie, Price Thea, Callahan Zachary, Yeo Charles J
Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania.
Department of Surgery, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania.
Case Rep Pancreat Cancer. 2016 Jun 1;2(1):53-57. doi: 10.1089/crpc.2016.0011. eCollection 2016.
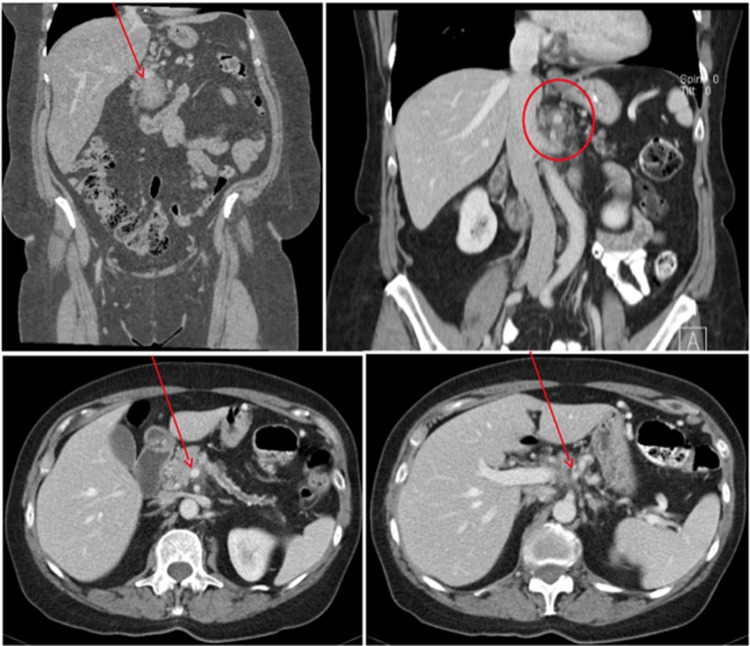
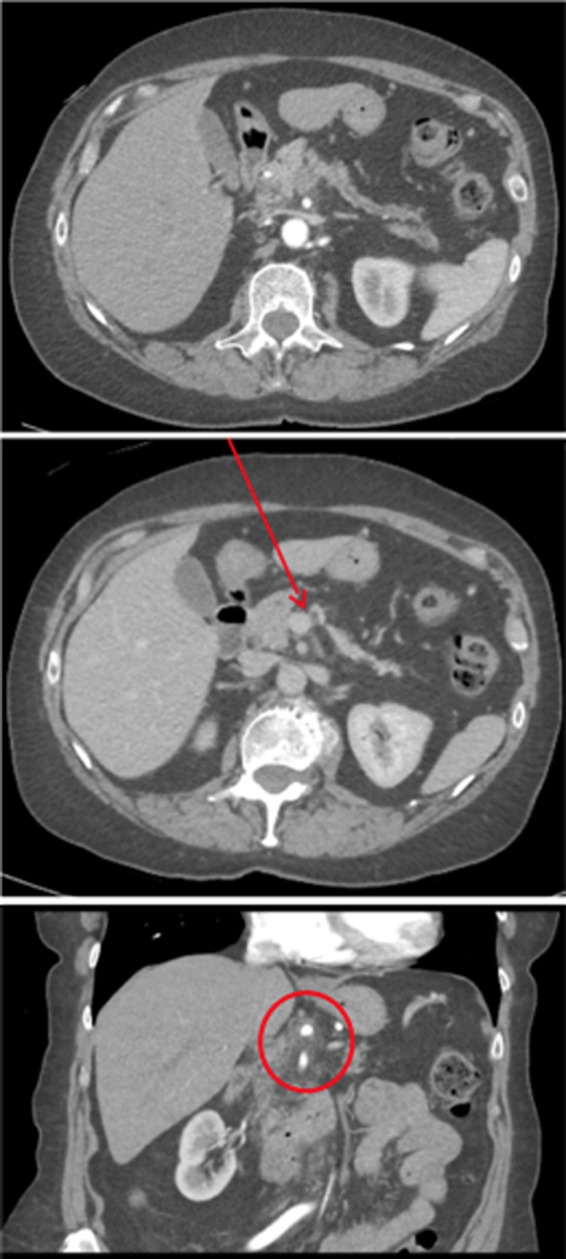
The modified Appleby procedure has been developed for cancer of the pancreatic body or tail with celiac axis invasion, historically classified as unresectable disease. Post-Appleby resection, the source of arterial blood to the liver is the superior mesenteric artery, which supplies the gastroduodenal artery and ultimately feeds the proper hepatic artery. In cases of inadequate collateralization, preoperative coiling of the common hepatic artery (CHA) or intraoperative reconstruction via an aorto-hepatic bypass has been described. We describe a 74-year-old female with a pancreatic mass that was initially determined to be unresectable. She underwent extensive combination neoadjuvant chemotherapy. A favorable response was evidenced by a decrease in serum CA 19-9 levels. After 7 months, she was restaged and offered a distal pancreatectomy (DP) with the possibility of a modified Appleby procedure due to potential tumor involvement of the proximal CHA. Intraoperatively, tumor was identified along the CHA traveling proximally to the celiac axis. Therefore, a modified Appleby procedure with DP and splenectomy was performed without the need for reconstruction of the CHA. Postoperative specimen pathology showed residual pancreatic ductal adenocarcinoma with marked treatment effects. The pathology confirmed an R0 resection. The patient followed our postpancreatic surgery care pathway. She remains well 7 months postoperatively. A pancreatic body or tail mass encasing the celiac vessels should not be an immediate referral for palliative care. Recent evidence shows that successful R0 resection can be achieved following neoadjuvant therapy. In fact, patients who have undergone a successful modified Appleby procedure show survival outcomes similar to patients with less advanced cancer who underwent standard DP. The modified Appleby procedure used in conjunction with neoadjuvant therapy can achieve complete resection in select patients previously thought to be unresectable.
改良的Appleby手术已被用于治疗侵犯腹腔干的胰体或胰尾癌,这类癌症在过去被归类为不可切除疾病。Appleby手术后,肝脏的动脉血供来源是肠系膜上动脉,该动脉供应胃十二指肠动脉,最终为肝固有动脉供血。在侧支循环不足的情况下,已有文献报道术前对肝总动脉(CHA)进行线圈栓塞或术中通过主动脉-肝旁路进行重建。我们报告一例74岁女性,其胰腺肿块最初被判定为不可切除。她接受了广泛的联合新辅助化疗。血清CA 19-9水平下降证明化疗反应良好。7个月后,她重新进行分期评估,并接受了远端胰腺切除术(DP),由于近端CHA可能受肿瘤累及,还可能进行改良的Appleby手术。术中,在CHA上发现肿瘤向近端延伸至腹腔干。因此,进行了改良的Appleby手术,包括DP和脾切除术,无需重建CHA。术后标本病理显示残留胰腺导管腺癌,有明显的治疗效果。病理证实为R0切除。患者遵循我们的胰腺手术后护理方案。术后7个月她情况良好。包绕腹腔血管的胰体或胰尾肿块不应立即转诊进行姑息治疗。最近的证据表明,新辅助治疗后可实现成功的R0切除。事实上,成功接受改良Appleby手术的患者的生存结果与接受标准DP的病情较轻癌症患者相似。改良的Appleby手术联合新辅助治疗可使部分先前被认为不可切除的患者实现完全切除。