Unit of Respiratory Medicine and Allergy, Department of Internal Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Unit of Occupational and Environmental Medicine, Department of Public Health and Community Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Respir Res. 2019 Jan 11;20(1):8. doi: 10.1186/s12931-019-0970-9.
Originally, studies on exhaled droplets explored properties of airborne transmission of infectious diseases. More recently, the interest focuses on properties of exhaled droplets as biomarkers, enabled by the development of technical equipment and methods for chemical analysis. Because exhaled droplets contain nonvolatile substances, particles is the physical designation. This review aims to outline the development in the area of exhaled particles, particularly regarding biomarkers and the connection with small airways, i e airways with an internal diameter < 2 mm.
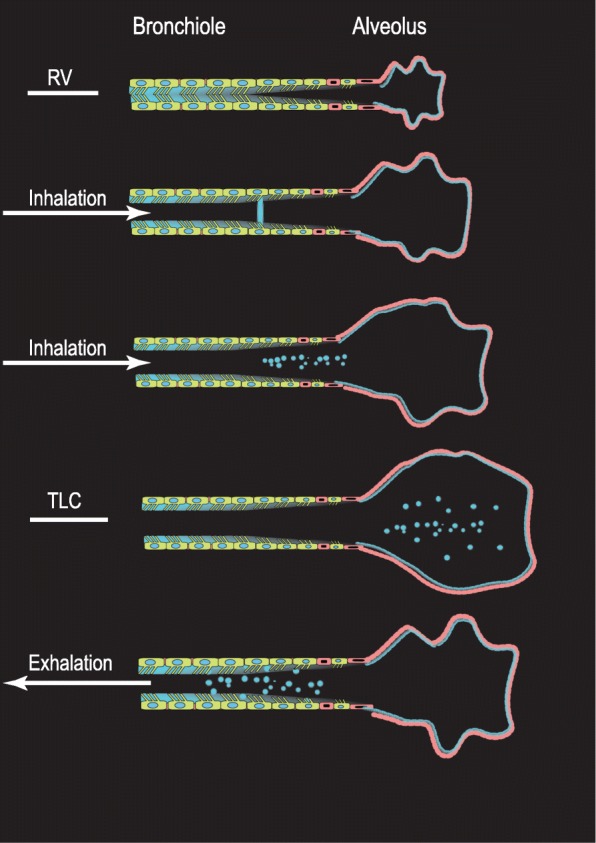
Generation mechanisms, sites of origin, number concentrations of exhaled particles and the content of nonvolatile substances are studied. Exhaled particles range in diameter from 0.01 and 1000 μm depending on generation mechanism and site of origin. Airway reopening is one scientifically substantiated particle generation mechanism. During deep expirations, small airways close and the reopening process produces minute particles. When exhaled, these particles have a diameter of < 4 μm. A size discriminating sampling of particles < 4 μm and determination of the size distribution, allows exhaled particle mass to be estimated. The median mass is represented by particles in the size range of 0.7 to 1.0 μm. Half an hour of repeated deep expirations result in samples in the order of nanogram to microgram. The source of these samples is the respiratory tract ling fluid of small airways and consists of lipids and proteins, similarly to surfactant. Early clinical studies of e g chronic obstructive pulmonary disease and asthma, reported altered particle formation and particle composition.
The physical properties and content of exhaled particles generated by the airway reopening mechanism offers an exciting noninvasive way to obtain samples from the respiratory tract lining fluid of small airways. The biomarker potential is only at the beginning to be explored.
最初,关于呼出飞沫的研究探索了传染病空气传播的特性。最近,由于开发了用于化学分析的技术设备和方法,人们对呼出飞沫作为生物标志物的特性产生了兴趣。由于呼出飞沫包含非挥发性物质,因此粒子是其物理名称。本篇综述旨在概述呼出粒子领域的发展,特别是关于生物标志物以及与小气道(即内径<2mm 的气道)的关系。
研究了呼出粒子的生成机制、起源部位、粒子数浓度和非挥发性物质含量。呼出粒子的直径范围为 0.01 至 1000μm,具体取决于生成机制和起源部位。气道再开放是一种有科学依据的粒子生成机制。在深呼气过程中,小气道关闭,再开放过程会产生微小的粒子。当这些粒子被呼出时,其直径<4μm。通过对直径<4μm 的粒子进行尺寸区分采样和确定其尺寸分布,可以估算出呼出粒子的质量。中位数质量由 0.7 至 1.0μm 范围内的粒子表示。反复深呼气半小时会产生纳克到微克数量级的样本。这些样本的来源是小气道的呼吸道黏膜液,其中包含与表面活性剂类似的脂质和蛋白质。早期的慢性阻塞性肺疾病和哮喘等临床研究报告了粒子形成和组成的改变。
气道再开放机制生成的呼出粒子的物理特性和内容为非侵入性地从小气道的呼吸道黏膜液中获取样本提供了一种令人兴奋的方法。生物标志物的潜力才刚刚开始被探索。