Ph.D. Program in Translational Medicine, Kaohsiung Medical University and Academia Sinica, Taiwan; Division of Nephrology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan; Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan; Faculty of Renal Care, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan; Neuroscience Program of Academia Sinica, Academia Sinica, Taipei, Taiwan.
EBioMedicine. 2019 Feb;40:675-684. doi: 10.1016/j.ebiom.2019.01.011. Epub 2019 Jan 11.
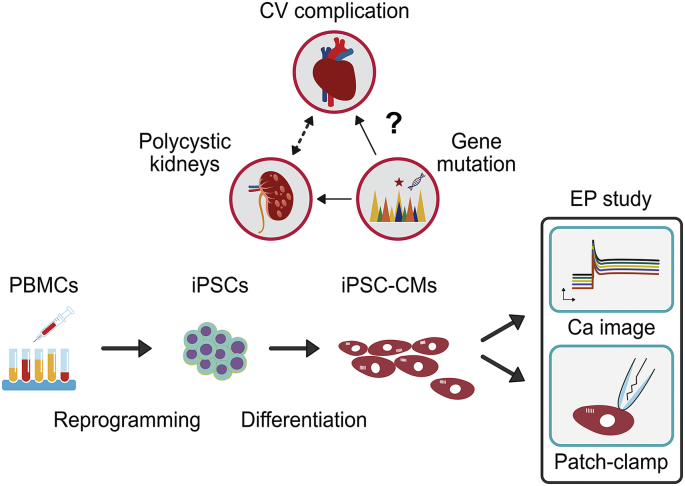
Mutations in PKD1 or PKD2 gene lead to autosomal dominant polycystic kidney disease (ADPKD). The mechanism of ADPKD progression and its link to increased cardiovascular mortality is still elusive.
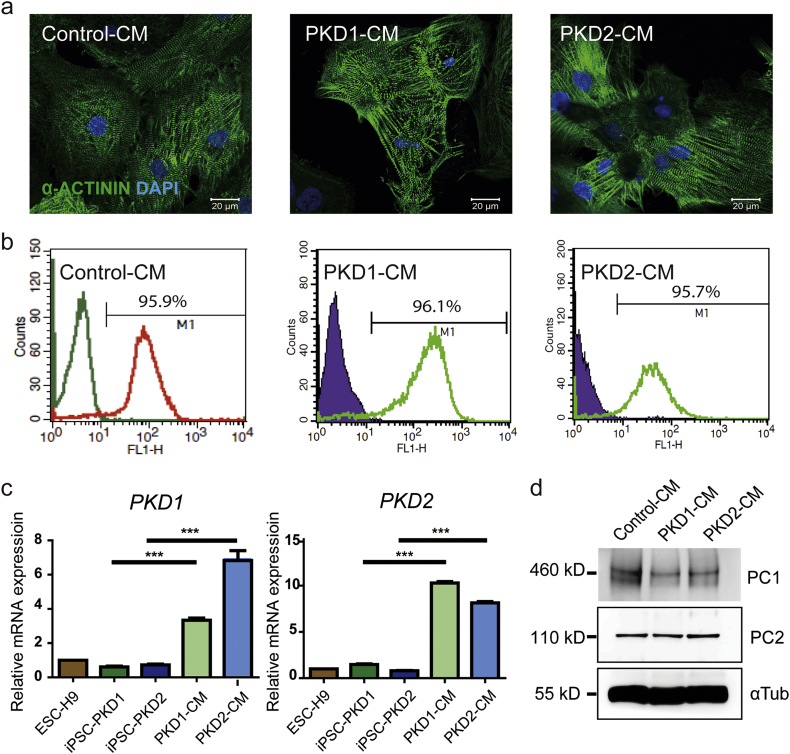
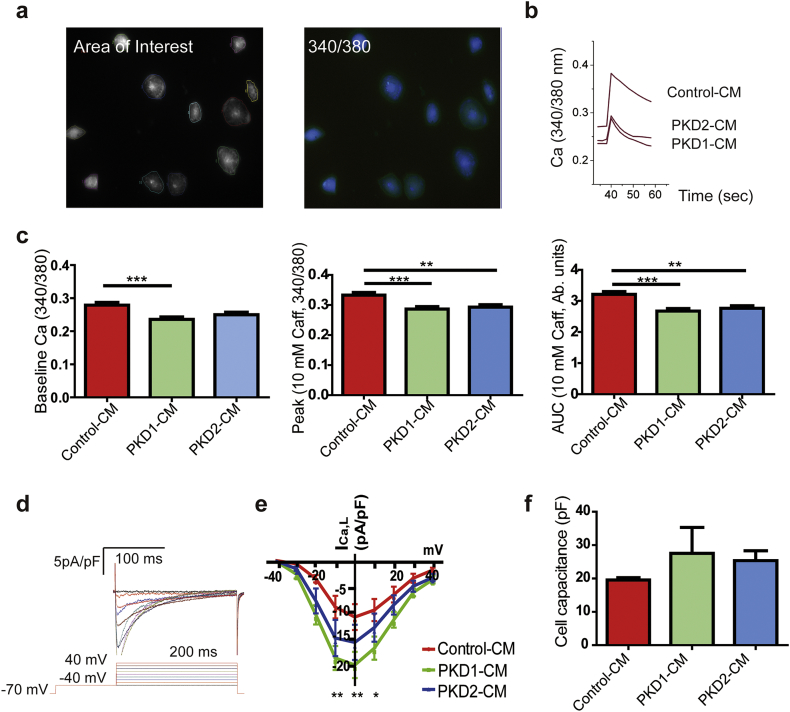
We differentiated ADPKD patient induced pluripotent stem cells (iPSCs) to cardiomyocytes (CMs). The electrophysiological properties at the cellular level were analyzed by calcium imaging and whole cell patch clamping.
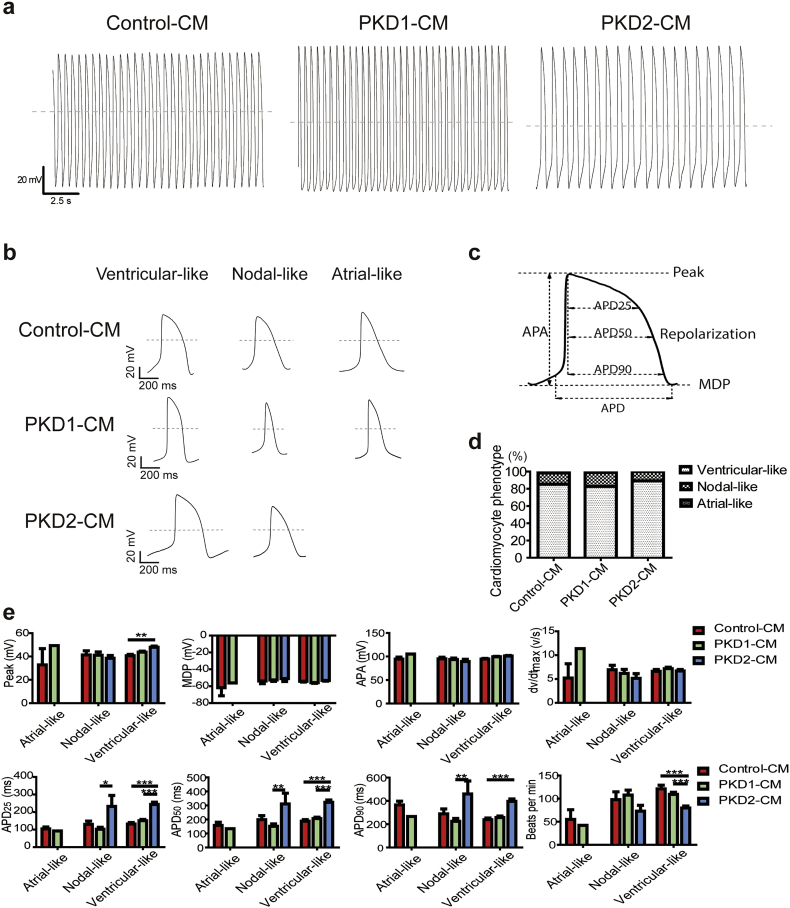
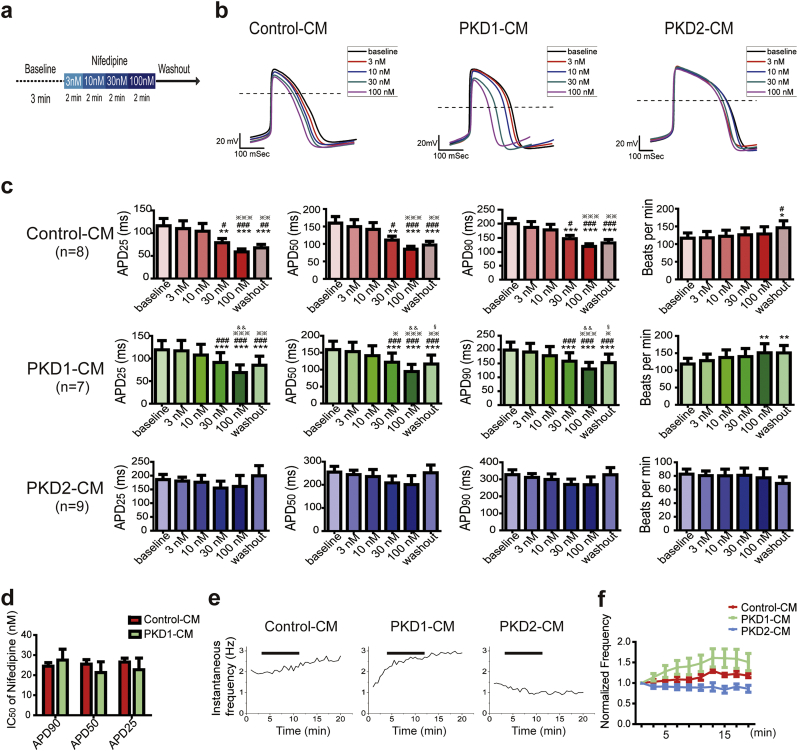
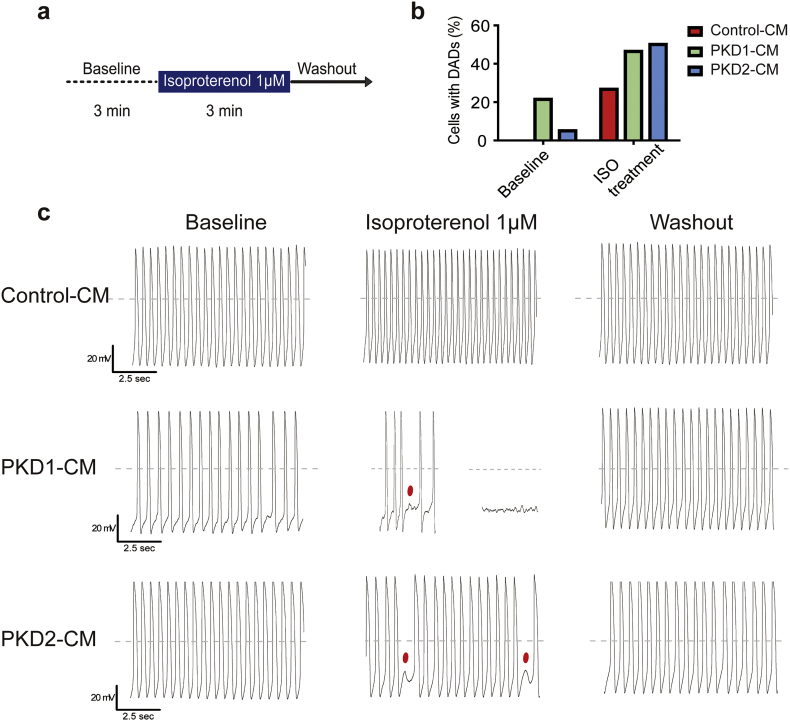
The ADPKD patient iPSC-CMs had decreased sarcoplasmic reticulum calcium content compared with Control-CMs. Spontaneous action potential of the PKD2 mutation line-derived CMs demonstrated slower beating rate and longer action potential duration. The PKD1 mutation line-derived CMs showed a comparable dose-dependent shortening of phase II repolarization with the Control-CMs, but a significant increase in beating frequency in response to L-type calcium channel blocker. The PKD1-mutant iPSC-CMs also showed a relatively unstable baseline as a greater percentage of cells exhibited delayed afterdepolarizations (DADs). Both the ADPKD patient iPSC-CMs showed more β-adrenergic agonist-elicited DADs compared with Control-CMs.
Characterization of ADPKD patient iPSC-CMs provides new insights into the increased clinical risk of arrhythmias, and the results enable disease modeling and drug screening for cardiac manifestations of ADPKD. FUND: Ministry of Science and Technology, National Health Research Institutes, Academia Sinica Program for Technology Supporting Platform Axis Scheme, Thematic Research Program and Summit Research Program, and Kaohsiung Medical University Hospital, Taiwan.
PKD1 或 PKD2 基因突变导致常染色体显性多囊肾病(ADPKD)。ADPKD 进展的机制及其与心血管死亡率增加的关系仍不清楚。
我们将 ADPKD 患者诱导多能干细胞(iPSC)分化为心肌细胞(CMs)。通过钙成像和全细胞膜片钳技术在细胞水平上分析电生理特性。
与对照 CM 相比,ADPKD 患者 iPSC-CM 的肌浆网钙含量降低。PKD2 突变系衍生的 CMs 的自发性动作电位显示出较慢的搏动率和较长的动作电位持续时间。PKD1 突变系衍生的 CMs 表现出与对照 CM 相似的剂量依赖性 II 期复极缩短,但对 L 型钙通道阻滞剂的搏动频率显著增加。PKD1 突变 iPSC-CM 也表现出相对不稳定的基线,因为更大比例的细胞表现出延迟后除极(DADs)。与对照 CM 相比,两种 ADPKD 患者 iPSC-CM 显示出更多的β-肾上腺素能激动剂诱发的 DADs。
ADPKD 患者 iPSC-CM 的特征为心律失常的临床风险增加提供了新的见解,结果可用于疾病建模和 ADPKD 心脏表现的药物筛选。
科技部、国家卫生研究院、中央研究院技术支持平台轴心计划、专题研究计划和高峰研究计划,以及台湾高雄医学大学附属医院。