Yu Yijin, Liu Nan, Zeng Qingxin, Duan Jing, Bao Qi, Lei Min, Zhao Jinning, Xie Junran
Department of Anesthesiology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Zhejiang, China,
Department of Anesthesiology, Hangzhou Xiasha Hospital, Zhejiang, China.
J Pain Res. 2018 Dec 28;12:159-170. doi: 10.2147/JPR.S183411. eCollection 2019.
Pregabalin is commonly used as an analgesic for neuropathic pain. But pregabalin as an adjunct to a multimodal analgesic regimen - although standard clinical protocol in some settings - has remained controversial. This meta-analysis was conducted to identify the efficacy of pregabalin for management of postoperative pain in thoracotomy.
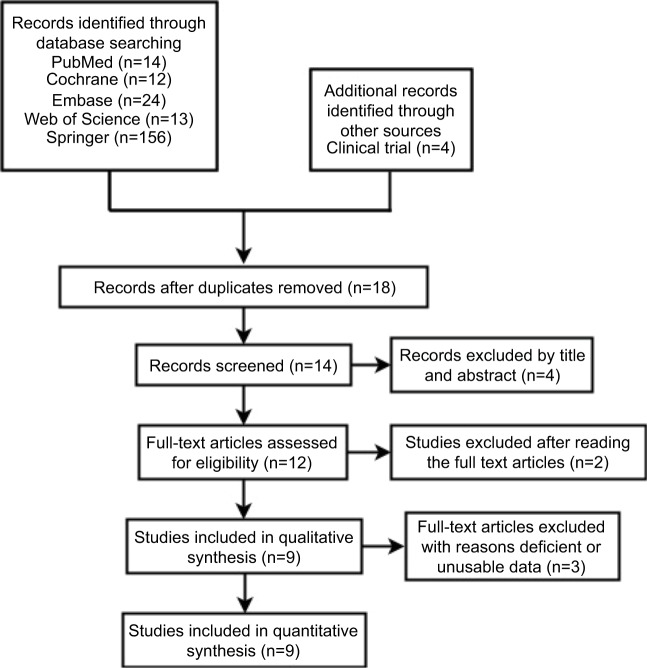
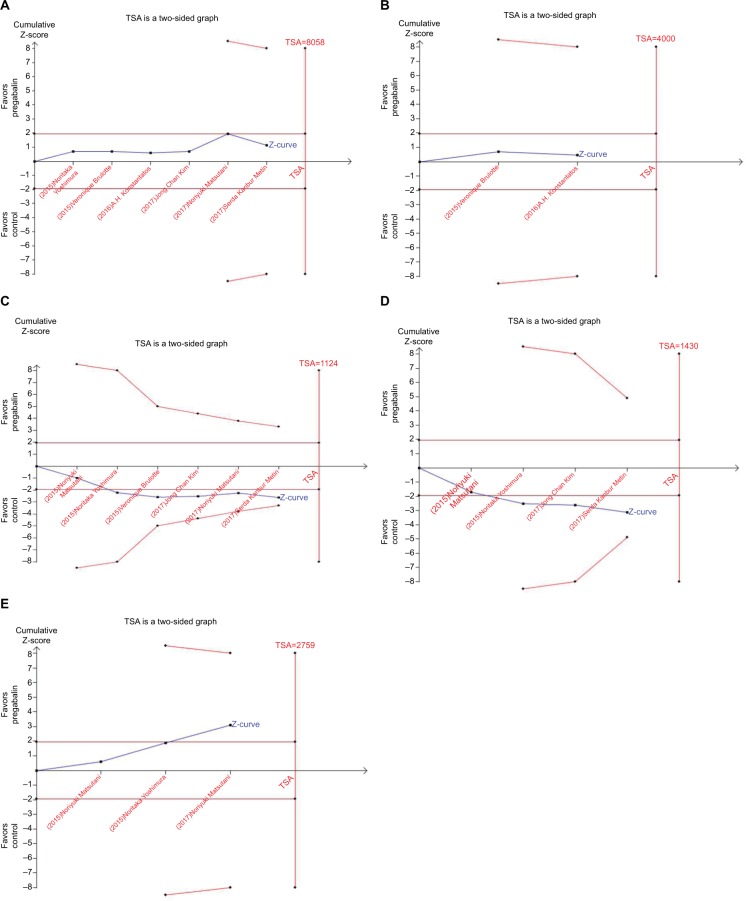
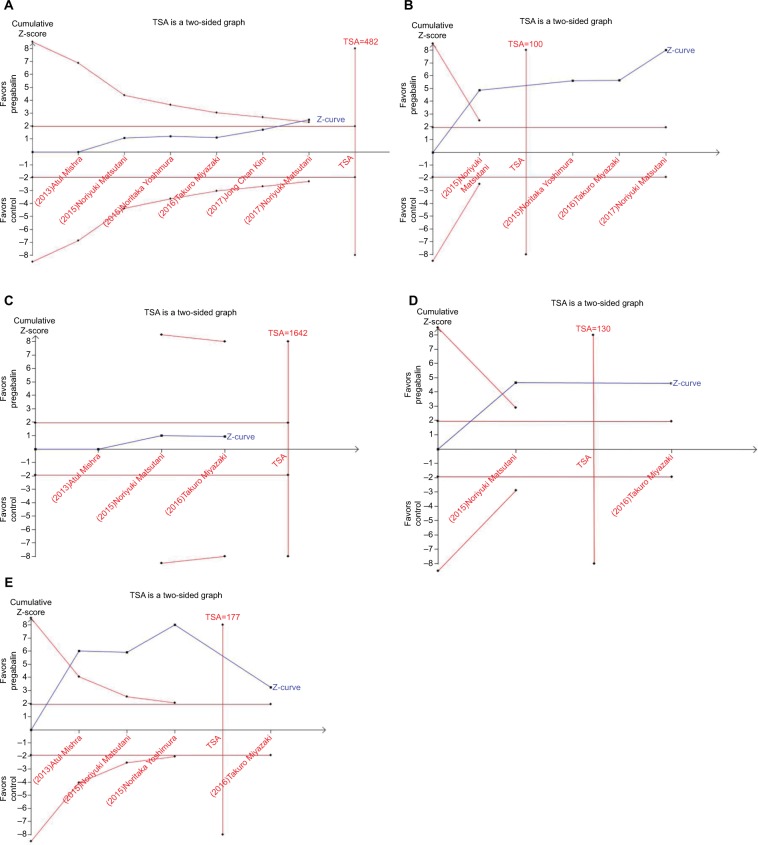
Pubmed, Embase, Cochrane, Web of Science, Springer, and Clinical Trial Register database were searched for randomized controlled trials (RCTs) of pregabalin in preventing postoperative pain in thoracotomy. Review Manager 5.3 and STATA 12.0 were selected to conduct the meta-analysis. Trial sequential analysis was used to control random errors and calculate the required information size.
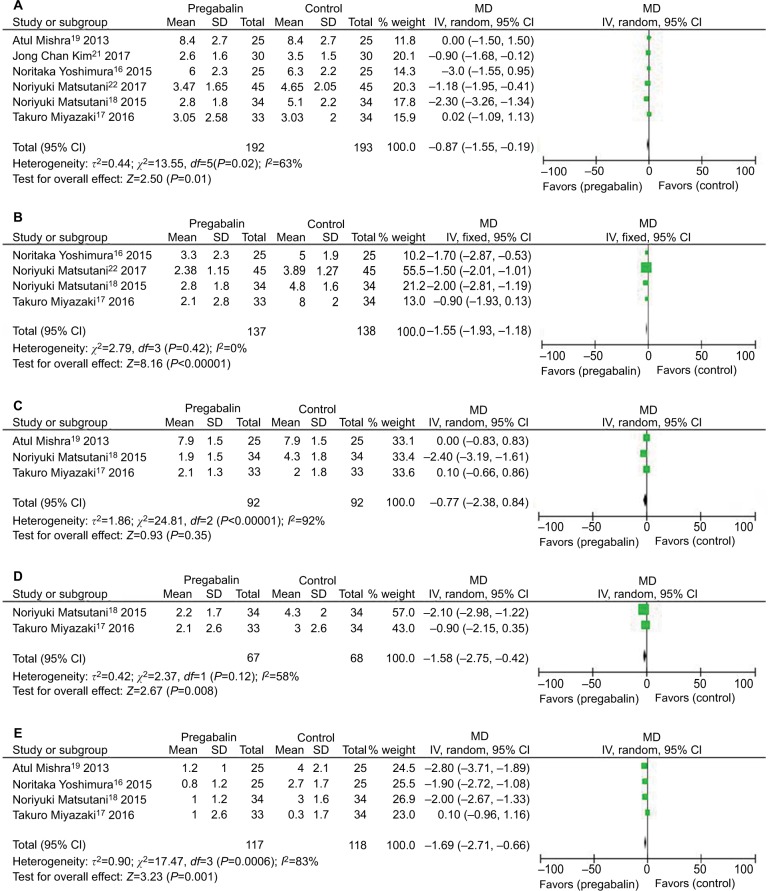
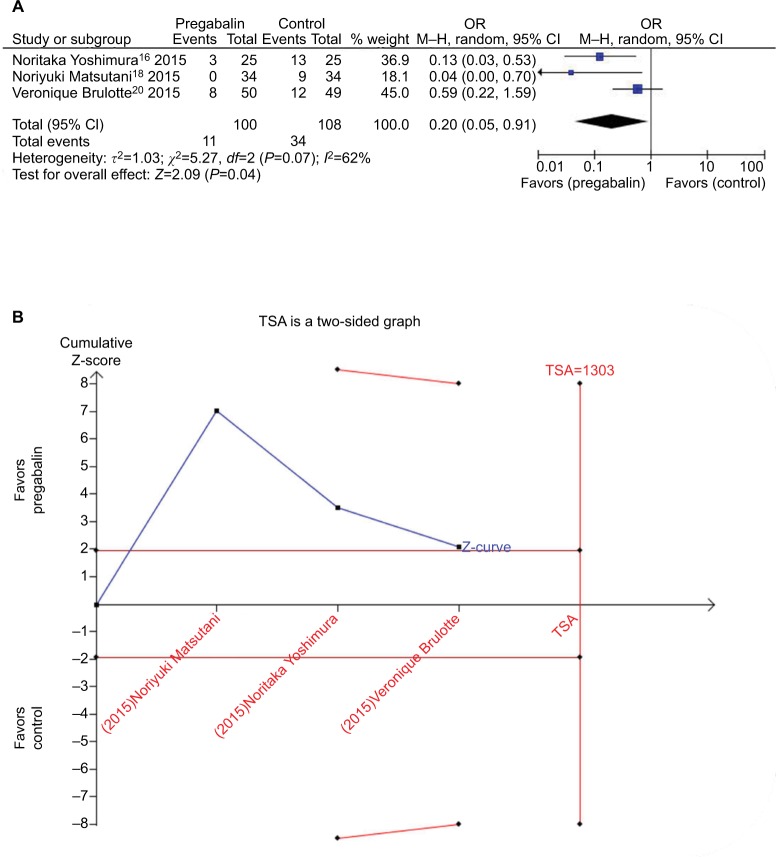
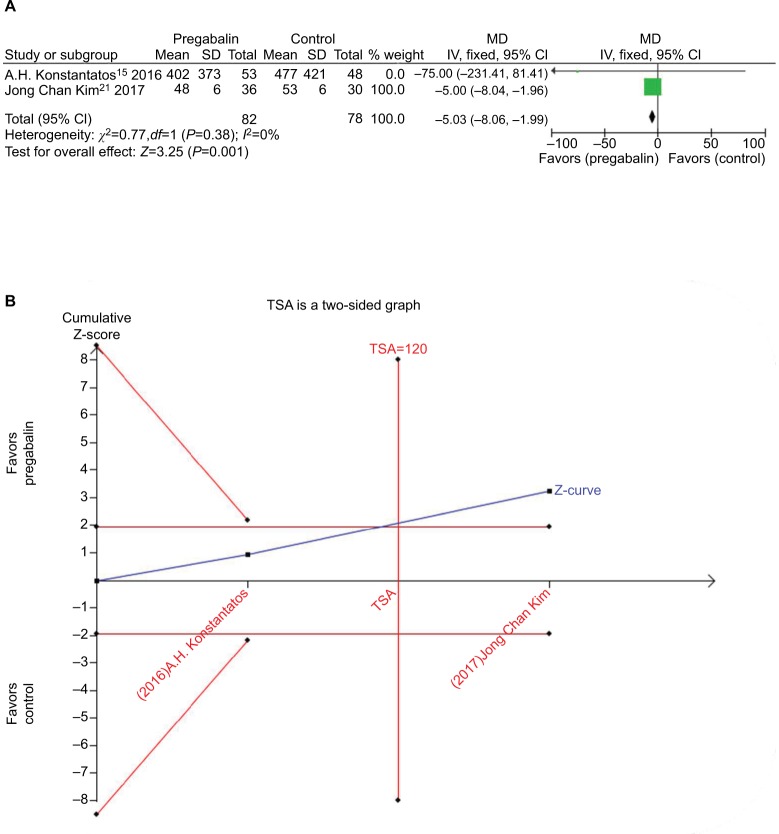
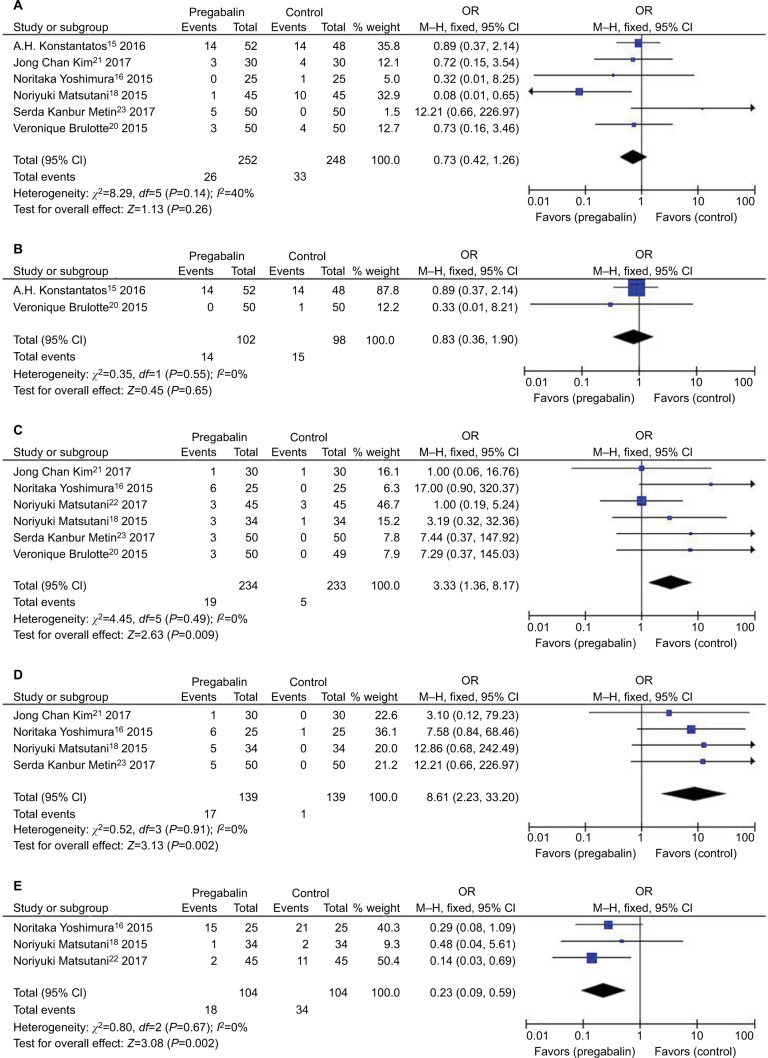
Nine RCTs with 684 patients were included in our meta-analysis. Outcomes favoring pregabalin included less pain on a 0-10 scale on 1 day [mean difference (MD): -0.87; 95% CI: -1.55 to -0.19; =0.01], 3 days (MD: -1.55; 95% CI: -1.93 to -1.18; <0.00001), 1 month (MD: -1.58; 95% CI: -2.75 to -0.42; =0.008), 3 months (MD: -1.69; 95% CI: -2.71 to -0.66; =0.001) postoperatively, and less incidence of neuropathic pain (OR: 0.20; 95% CI: 0.05-0.91; =0.04), less mean morphine consumption (MD: -5.03; 95% CI: -8.06 to -1.99; =0.001), but more dizziness (OR: 3.33; 95% CI: 1.36-8.17; =0.009), more drowsiness (OR: 8.61; 95% CI: 2.23-33.20; =0.002), and less constipation (OR: 0.23; 95% CI: 0.09-0.59; =0.002). There was no statistical differences in pain score on 7 days (MD:-0.77; 95% CI: -2.38 to 0.84; =0.35), nausea (OR: 0.73; 95% CI: 0.42-1.26; =0.26), and vomiting (OR: 0.83; 95% CI: 0.36-1.90; =0.65).
Pregabalin can prevent postoperative pain in thoracotomy and decrease incidence of neuropathic pain and morphine consumption. Pregabalin may be a valuable asset in management of acute and persistent postoperative pain in thoracotomy.
普瑞巴林常用于治疗神经性疼痛。但普瑞巴林作为多模式镇痛方案的辅助药物——尽管在某些情况下是标准临床方案——仍存在争议。本荟萃分析旨在确定普瑞巴林对开胸术后疼痛的管理效果。
检索了PubMed、Embase、Cochrane、Web of Science、Springer和临床试验注册数据库,以查找普瑞巴林预防开胸术后疼痛的随机对照试验(RCT)。选择Review Manager 5.3和STATA 12.0进行荟萃分析。采用试验序贯分析来控制随机误差并计算所需信息量。
我们的荟萃分析纳入了9项RCT,共684例患者。支持普瑞巴林的结果包括术后1天0-10分疼痛评分更低(平均差[MD]:-0.87;95%置信区间:-1.55至-0.19;P=0.01)、3天(MD:-1.55;95%置信区间:-1.93至-1.18;P<0.00001)、1个月(MD:-1.58;95%置信区间:-2.75至-0.42;P=0.008)、3个月(MD:-1.69;95%置信区间:-2.71至-0.66;P=0.001),神经性疼痛发生率更低(比值比[OR]:0.20;95%置信区间:0.05-0.91;P=0.04),平均吗啡消耗量更低(MD:-5.03;95%置信区间:-8.06至-1.99;P=0.001),但头晕更多(OR:3.33;95%置信区间:1.36-8.17;P=0.009),嗜睡更多(OR:8.61;95%置信区间:2.23-33.20;P=0.002),便秘更少(OR:0.23;95%置信区间:0.09-0.59;P=0.002)。术后7天疼痛评分(MD:-0.77;95%置信区间:-2.38至0.84;P=0.35)、恶心(OR:0.73;95%置信区间:0.42-1.26;P=0.26)和呕吐(OR:0.83;95%置信区间:0.36-1.90;P=0.65)无统计学差异。
普瑞巴林可预防开胸术后疼痛,降低神经性疼痛发生率和吗啡消耗量。普瑞巴林可能是管理开胸术后急性和持续性疼痛的宝贵药物。