HSR&D Research Enhancement Award Program and Geriatrics Research, Education, and Clinical Center, James J. Peters Veterans Administration Medical Center, Bronx, NY 10468, USA.
Med Care. 2010 Jul;48(7):652-8. doi: 10.1097/MLR.0b013e3181dbe35d.
The Centers for Medicare and Medicaid Services (CMS) publicly reports hospital-specific risk-standardized, 30-day, all-cause, mortality rates (RSMRs) for all hospitalizations among fee-for-service Medicare beneficiaries for acute myocardial infarction (AMI), heart failure (HF), and pneumonia at non-Federal hospitals.
To examine the performance of the statistical models used by CMS among veterans at least 65 years of age hospitalized for AMI, HF, and pneumonia in Veterans Health Administration (VHA) hospitals.
Cross-sectional analysis of VHA administrative claims data between October 1, 2006 and September 30, 2009.
Thirteen thousand forty-six veterans hospitalized for AMI among 123 VHA hospitals; 26,379 veterans hospitalized for HF among 124 VHA hospitals; and 31,126 veterans hospitalized for pneumonia among 124 VHA hospitals.
Hospital-specific RSMR for AMI, HF, and pneumonia hospitalizations calculated using hierarchical generalized linear models.
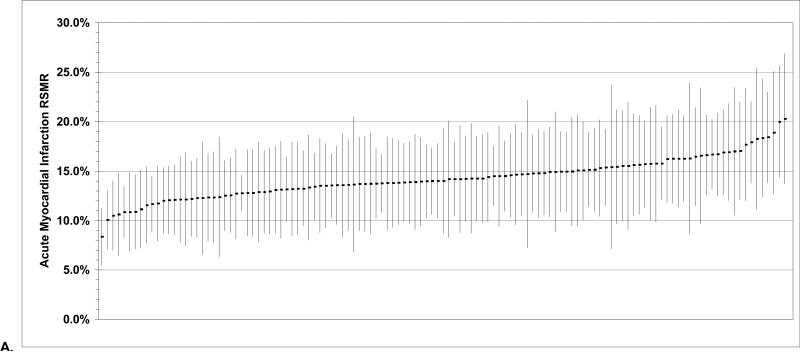
Median number of AMI hospitalizations per VHA hospital was 87. Average AMI RSMR was 14.3% [95% confidence interval (CI), 13.9%-14.6%] with modest heterogeneity among VHA hospitals (RSMR range: 8.4%-20.3%). The c-statistic for the AMI RSMR statistical model was 0.79. Median number of HF hospitalizations was 188. Average HF RSMR was 10.1% (95% CI, 9.9%-10.4%) with modest heterogeneity (RSMR range: 6.1%-14.9%). The c-statistic for the HF RSMR statistical model was 0.73. Median number of pneumonia hospitalizations was 221.5. Average pneumonia RSMR was 13.0% (95% CI, 12.7%-13.3%) with modest heterogeneity (RSMR range: 9.0%-18.4%). The c-statistic for the pneumonia RSMR statistical model was 0.72.
The statistical models used by CMS to estimate RSMRs for AMI, HF, and pneumonia hospitalizations at non-Federal hospitals demonstrate similar discrimination when applied to VHA hospitals.
医疗保险和医疗补助服务中心(CMS)公开报告了非联邦医院服务项目下,医疗保险受益人的急性心肌梗死(AMI)、心力衰竭(HF)和肺炎住院患者的特定医院风险标准化、30 天全因死亡率(RSMR)。
检查 CMS 在退伍军人健康管理局(VHA)医院对至少 65 岁的 AMI、HF 和肺炎住院退伍军人使用的统计模型的性能。
2006 年 10 月 1 日至 2009 年 9 月 30 日的 VHA 行政索赔数据的横断面分析。
123 家 VHA 医院 13046 名 AMI 住院退伍军人;124 家 VHA 医院 26379 名 HF 住院退伍军人;124 家 VHA 医院 31126 名肺炎住院退伍军人。
使用分层广义线性模型计算 AMI、HF 和肺炎住院患者的特定医院 RSMR。
每家 VHA 医院 AMI 住院人数中位数为 87。AMI 的平均 RSMR 为 14.3%(95%置信区间,13.9%-14.6%),VHA 医院之间存在适度的异质性(RSMR 范围:8.4%-20.3%)。AMI RSMR 统计模型的 c 统计量为 0.79。HF 住院人数中位数为 188。HF 的平均 RSMR 为 10.1%(95%置信区间,9.9%-10.4%),异质性适度(RSMR 范围:6.1%-14.9%)。HF RSMR 统计模型的 c 统计量为 0.73。肺炎住院人数中位数为 221.5。肺炎的平均 RSMR 为 13.0%(95%置信区间,12.7%-13.3%),异质性适度(RSMR 范围:9.0%-18.4%)。肺炎 RSMR 统计模型的 c 统计量为 0.72。
CMS 用于估计非联邦医院 AMI、HF 和肺炎住院患者 RSMR 的统计模型在应用于 VHA 医院时表现出相似的区分度。